by Sara Giarnieri, September 21, 2021
It’s no secret that the fashion industry controls a big part of our media consumption. We see it in movies, clothing websites, advertisements, and other platforms. However, fashion isn’t as beautiful as it seems in its deceiving haute couture shows and eye-catching magazines; it is a dark industry. The fashion industry is sexist because of the workplace ‘glass ceiling’, sexual objectification, and its influence on disordered eating, making it an industry of little mobility and a lot of exploitation.
The ‘glass ceiling’ of the fashion industry is a persisting problem. It is hard for women to obtain higher roles in the workplace. According to “Shattering the Glass Runway,” a 2018 report by Pamela Brown, Stacey Haas, Sophie Marchessou, and Cyrielle Villepelet, only “14 percent of major brands have a female executive in charge” (Brown et al.). This number is concerningly low considering that “70 percent of women aspire to become top executives, versus 60 percent of men” (Brown et al.). More women want to achieve those higher roles in the workplace than men, yet less than 15% of women actually have those roles in top fashion brands. According to the article, women are prevented from achieving these positions because of lack of advice from senior colleagues, lack of promotions, and childcare burdens at home, as women are expected to play a larger role in caretaking for their children (Brown et al.). Women should be able to provide insight on certain things that men may not know, such as size-inclusivity for clothing or wider shade ranges for undergarments, but they are stuck in less influential roles. For an industry that is so heavily marketed towards women, there aren’t many women that represent the industry.
Another problem in the fashion industry is its sexual objectification of women, often to appease the male eye. According to “Disordered Eating Behaviors and Sexual Objectification during New York Fashion Week: Implementation of Industry Policies and Legislation” (2020), female models experience sexual harassment and invasion of privacy: a study surveyed 76 models, 87 percent of them female, that participated in New York Fashion Week in the Fall of 2018 (Austin et al.). Of the 76 participants, 32 said that they “experienced invasive photography or lack of privacy while changing backstage” (Austin et al.). It is clear that the basic human need for privacy is not respected in the fashion industry. Sexual harassment in the fashion industry needs to be addressed. It is illegal, and it is morally wrong.
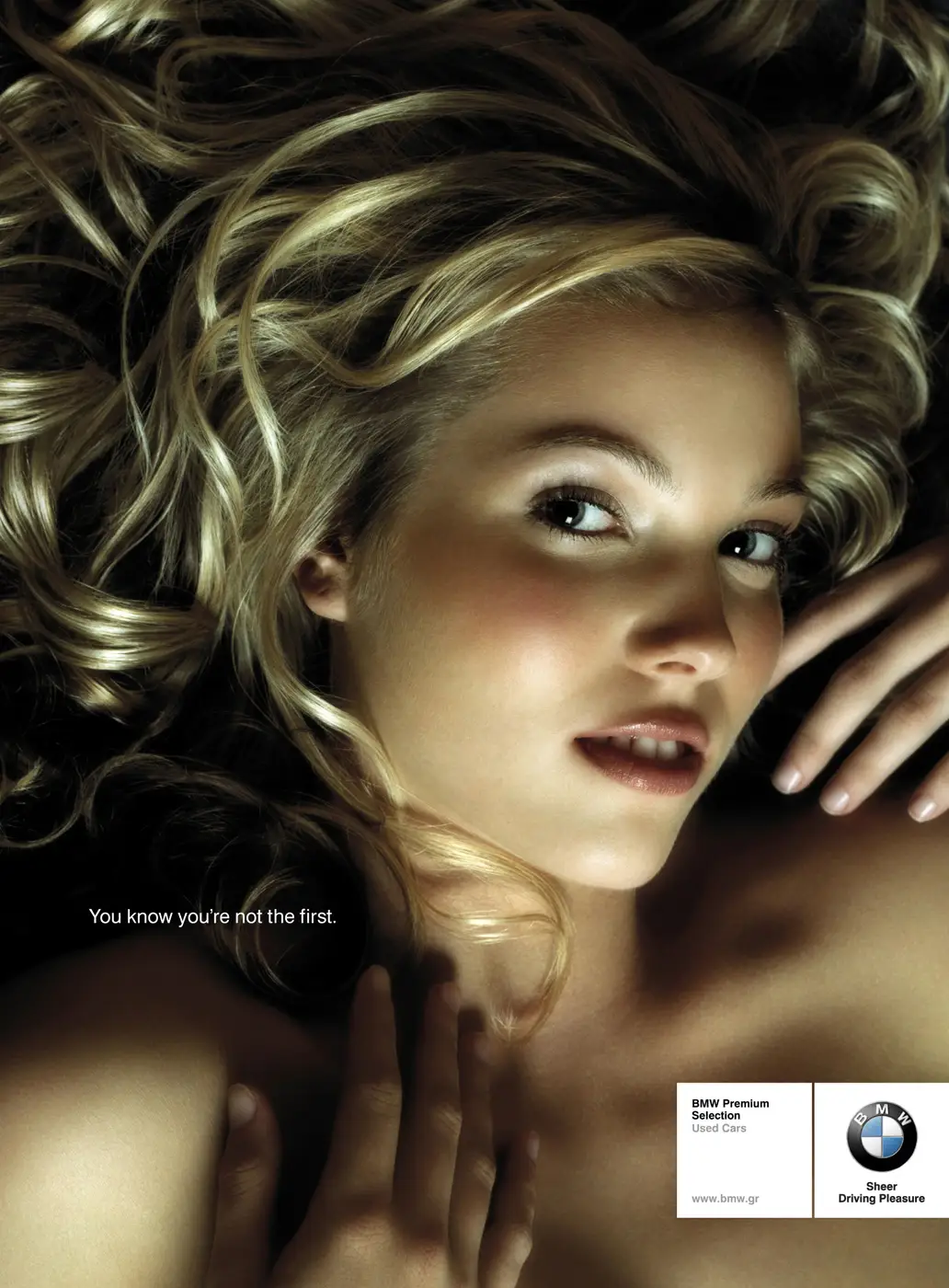
Objectification of women also stems from advertisements and campaigns. A 2019 article posted by FashionHarp called “Hyper Sexualization in the Fashion Industry” highlights the oversexualization of women in brands like Dolce & Gabbana and Vogue. They also emphasize the racism that black women experience through their portrayal as “wild, sexual beasts that just can’t seem to shed their animalistic spots” in many of their sexualized photos (“Hyper Sexualisation in the Fashion Industry”). This objectification of women is harmful to display for the public, as it insinuates that women should be treated as such, making the important progress of feminist movements backpedal. The racist and sexual portrayal of black women as animals is also a huge issue that needs to be acknowledged. Equality has been growing for decades, shutting down prejudices and unfairness along the way. Why hasn’t the fashion industry done so as well? Presenting black women as “animalistic” is a negative stereotype that needs to be left behind in order to truly be inclusive. The industry, rather than simply focusing on fashion, finds a need to simultaneously objectify women in the process.
Lastly, the fashion industry pushes such unrealistic beauty standards that many women are pressured into developing eating disorders. Disordered eating can happen to anyone, but in the fashion industry, it is prominently something women must battle. Many female models are forced to stay “slim,” thus creating long term unhealthy relationships with food. Looking back on the 2018 New York Fashion Week study, it was reported that in order to lose weight during the event, participants were “skipping meals, exercising, using fasts/cleanses/nutritional detoxes, using weight‐loss supplements or diet pills, using stimulants such as Ritalin, using intravenous drips such as “banana bags,” self‐induced vomiting, or other methods” (Austin et al.). The pressure to lose weight in the fashion industry comes with dangerous consequences, as shown by the concerning behaviors reported in the survey. Another concerning statistic is that “20% reported that an industry professional had suggested that their weight/shape had prevented them from booking a job” (Austin et al.), which further shows how big a factor weight is in the fashion industry.
In addition, Vogue uploaded a video directed by Shaina Danziger in 2019 called “9 Models on the Pressure to Lose Weight and Body Image,” as a part of their docu-series The Models. Ali Michael, an American model, recalled a past experience and said, “I went to Paris, and after the first day of castings my agency told me that the response from my first day of castings foreshows us that I had gained too much weight and was unusable for the shows” (Danziger). The emphasis on weight is alarming, as it could cause self-confidence issues amongst models or even amongst women in the general public watching this unfold. A few comments such as this on the video also raise some points of concern: “I’m confused about why Vogue is interviewing them & posting this… when they’re a part of the problem” (I Can Relate). It certainly feels hypocritical that Vogue is giving models a platform to talk about their body image issues in the industry while simultaneously causing these issues. If Vogue’s intention is to make a change, they have to practice what they preach.
Now, the question is: how do we combat sexism in the fashion industry? Spreading awareness is a significant first step in combating sexism. According to “Shattering the Glass Runway,” “100% of the women surveyed see gender inequality as an issue in fashion, while less than 50% of men do” (Brown et al.). It is clear that many people don’t seem to be aware of gender inequality, especially males in CEO fashion industry positions that look to exploit women for the sake of fortune. It is likely because they are in a better position in the industry that makes it hard to imagine the other side’s difficulties. If more statistics, studies, and personal stories regarding females in the fashion industry were publicized, maybe the heteropatriarchal perspective on inequality will change. Sexual harassment in the industry needs to be further exposed. Women, as well as anyone else, deserve to be protected and respected. Consequences regarding disordered eating need to be spread, sharing the disturbing numbers of people who suffer from disordered eating and showing how it affects health.
Though there is some effort to try and change the fashion industry, much more progress is needed. There are not enough resources out there to transform the fashion industry into something that promotes equality. A memo to the fashion industry: women are not objects, not toys, and not inferiors. Respect is something that everyone deserves. As people unveil the horrors you hide, more will start to change. Women will gain the respect that you fail to show.
Works Cited
Brown, Pamela, et al. “Shattering the Glass Runway.” McKinsey & Company, 19 Feb. 2019, http://www.mckinsey.com/industries/retail/our-insights/shattering-the-glass-runway#.
Danziger, Shaina. “9 Models on the Pressure to Lose Weight and Body Image | The Models | Vogue.” YouTube, uploaded by Vogue, 23 Apr. 2019, http://www.youtube.com/watch?v=MKd38G338Qw.
“Hyper Sexualisation in the Fashion Industry.” FashionHarp, 13 Feb. 2019, fashionharp.com/promotions/hyper-sexualisation-in-the-fashion-industry/.
I Can Relate. Comment on “9 Models on the Pressure to Lose Weight and Body Image | The Models | Vogue.” Youtube, http://www.youtube.com/watch?v=MKd38G338Qw.
Rodgers, Rachel, et al. “Disordered Eating Behaviors and Sexual Objectification during New York Fashion Week: Implementation of Industry Policies and Legislation.” International Journal of Eating Disorders, vol. 54, no. 3, Mar. 2021, pp. 433–437. EBSCOhost, doi:10.1002/eat.23432.