My central guiding question is “how can the impact of Audre Lorde as a catalyst for women’s liberation be itemized?” This question can be answered by examining Poet Audre Lorde’s work in the Women’s Liberation Movement during the late 1960s going into 1980. Audre Lorde (1934-1992) championed equality through her work as a Black lesbian cancer survivor and mother (Brandman, n.d.). She was a daughter of immigrants and was cognizant of issues in systems of oppression including racism, sexism, classism, and homophobia (Poetry Foundation, 2020). Lorde’s early works, including those discussed in the accompanying presentation, were the roots of her cumulative contributions to feminist theory, critical race studies, and commitment to inclusivity. Her words existed as a response to the second wave of the feminist movement during the 1960s and 1970s. This second wave was intended to help women pivot into roles beyond the private sphere and into the public sphere (Kang et al., 2017). This included motions for women to join more predominantly male workspaces and positions. Birth control and reproductive justice were also significant aspects of the second wave.
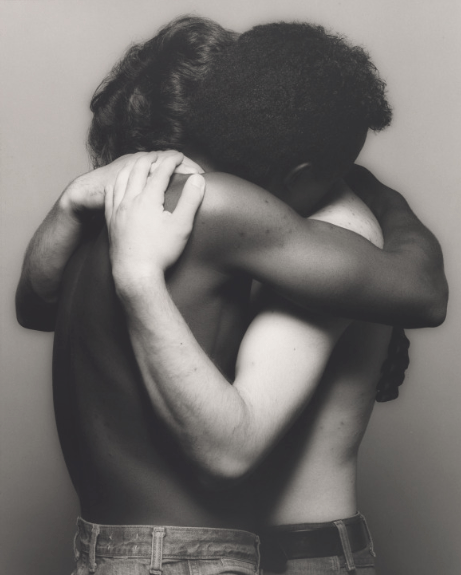
Lorde, seeing that the challenges affecting BIPOC women were not at the forefront of (or even close to) the movement’s agenda, decided to empower women of underrepresented and marginalized communities. The women she hoped to help were the same ones who were taught that their needs were not as important as the needs of the white middle-to-upper class women that the second wave embraced (Aviles, 2019). Lorde outright criticized the flagrant discrimination against BIPOC individuals in systems of injustice (Veaux, 2006). Audre Lorde was similar to other Black feminists in that she not only advocated for women’s rights but also fought for equality within the Black liberation movement. She enabled others to change their own futures on a national scale. Lorde is unique in that her vessel of change was her poetry and she focused on her battle with breast cancer as opposed to reproductive health. With respect to her LGBTQ+ advocacy, she was unapologetic for defying heteronormative standards in addition to beauty standards for what was considered feminine.
In contemporary media culture, the more information we get and the faster we get it, the more satisfied we are. But at some point, we have to consider the consequences of sharing too much about ourselves. Oversharing is when someone excessively broadcasts personal information over social media.
What kind of information can be overshared?
A prime example is location—where you are and who you are with. Most social media platforms enable users to share location. For some platforms, location sharing has to be done manually by the individual. On Instagram, you can make a post and tag your location, so everyone who sees your posts can see where you are. On the other hand, sometimes your location is shared simply by using the app. For instance, if you enable the map feature on Snapchat, your followers can see where you are whenever you open the app again.
Another example of overshared information is family information. Family information includes birthdays, names of siblings and parents, or major family events (like a family member moving into a new house). Social media has its advantages in that it connects families and friends. However, posting family information becomes an act of oversharing if you let the public know the details of your family dynamics or personal information.
A third form of oversharing is indulging your followers with your personal thoughts and emotions. A study published in 2017 calls this “self-disclosure” because you are voluntarily disclosing your inner sentiments to the world (Zhang, 527). In these situations, an individual uses social media to convey their mental state to the public. Often, this happens spontaneously and in the heat of the moment. For example, a user may negatively comment on people they know such as coworkers or make an impassioned statement involving politics.
A fourth form of oversharing is sharing the private conversations you have with others. This can be done by screenshotting direct messages and then posting these conversations elsewhere. For example, you can screenshot text messages with one person and then share this screenshot on Snapchat for your followers to see. This is oversharing because you would be violating the trust of the person you were having the private conversation with. By sharing private messages on social media, you are in effect, allowing others to eavesdrop on your conversation. You consented to this because you were the one who shared the conversation, but the others involved in the conversation may not have.
Virtually any social media app allows for oversharing. This is because social media is inherently made for sharing information. The complication is that social media has become so advanced that information can be shared more easily. If you overshare information about yourself (such as your location), this may be considered primary overshared information because it’s about you. However, if you overshare information about someone else (like their birthday, or their child’s name, or a private message you received from them), this may be considered secondary overshared information because you are revealing information about someone else via social media.
Why do people overshare?
A prominent reason is stress sharing. A study found that adolescents may feel inclined to overshare information because it gives them a sense of freedom (Radovic et al. 7). There may be a variety of circumstances in a person’s life that make them depressed and bogged down, but being able to post whatever they want on social media grants some sense of freedom. It is a form of expression.
In addition, the urge to overshare may be triggered when a user observes something on social media that incites them into posting a passionate retort (Radovic et al. 10). We can think of politics as a prime example of sensitive subject matter that may trigger people to overshare their emotions.
We should also consider that people may overshare to seek attention. This is more complicated, because attention-seeking behavior may be the result of narcissism, or simply because someone is genuinely seeking help. In the former case, a person may overshare information about themselves to brag, or they might overshare information about others at the expense of other people’s privacy. On the other hand, if a person is genuinely seeking help, they may overshare information about themselves in order to attract the right support groups (Newman et al. 344; Zhang, 527). The more information they share about themselves, the more likely people will come to their aid and give positive reinforcement.
Goal-setting and a competitive spirit are also reasons people will overshare on social media (Munson and Consolvo, 26). People are more likely to achieve their goals if they make their goals public and well-known. A study has found that a person’s motivation increases if they believe their goals are known by people they deem to be superior (Klein et al. 372). For example, in college, there is a lot of competition and students may feel compelled to overshare their goals in order to increase their motivation to accomplish them.
Lastly, people may overshare in order to create a perfected persona of themselves. In one study, a participant displayed a lot of her athletic information on social media, including many pictures and statistics, because it helped her create a new brand for herself (Newman et al. 346).
What are the consequences?
The first consequence of oversharing is putting yourself in danger. This can be in the form of robbery or stalking (Velempini and Nyoni, 4). If you overshare your location, daily routine, and social activities, people can track you and have a good idea of where you will be and when. This happened to social media influencer and entrepreneur Kim Kardashian in 2016, when thieves reportedly used Kardashian’s social media activity to find her location in Paris and confirm when she was alone. With this information, they broke into her residence, restrained her, and robbed her.
Another consequence is damaging your professional prospects. If you decide to go on a rant on social media about your employer, you can be held responsible for whatever you say, because after all, you decided to post it. If your post is discovered by a colleague or your employer, you could potentially lose your job.
In terms of reputation, some things are better left private, and oversharing can cause your private and public lives to collide. For example, Jeff Bezos, the founder of Amazon, had personal texts with his girlfriend released to the public. Reportedly, it happened because his girlfriend shared screenshots of their conversation with her brother. While Bezos didn’t lose his job, he went through public embarrassment as a result of his girlfriend’s oversharing.
How do we avoid oversharing?
Avoid posting on social media when you’re angry. Your judgment will be clouded, and your overshared information may not represent you at your best. Double check your privacy settings. If you want to post things like family-related content, make sure only close friends and family can see it, not the general public. Lastly, when crafting a social media post, be mindful of who sees your posts. But remember, people can always screenshot your posts and share it elsewhere, so take that into consideration. Unfortunately, private information doesn’t always stay private, but taking the steps outlined above as precautionary measures may lessen the likelihood of risky oversharing in a growing digital world.
Works Cited
Klein, Howard J., et al. “When Goals Are Known: The Effects of Audience Relative Status on Goal Commitment and Performance.” Journal of Applied Psychology, vol. 105, no. 4, 2020, pp. 372–389., doi.org/10.1037/apl0000441.
Munson, Sean and Sunny Consolvo. “Exploring Goal-Setting, Rewards, Self-Monitoring, and Sharing to Motivate Physical Activity.” Proceedings of the 6th International Conference on Pervasive Computing Technologies for Healthcare, 3 July 2012, pp. 25–32., doi.org/10.4108/icst.pervasivehealth.2012.248691.
Newman, Mark, et al. “It’s Not That I Don’t Have Problems, I’m Just Not Putting Them on Facebook: Challenges and Opportunities in Using Online Social Networks for Health.” Proceedings of the ACM 2011 Conference on Computer Supported Cooperative Work, Association for Computing Machinery, March 2011, pp. 341–50, doi.org/10.1145/1958824.1958876.
Radovic, Ana, et al. “Depressed Adolescents’ Positive and Negative Use of Social Media.” Journal of Adolescence, vol. 55, 2017, pp. 5–15., doi.org/10.1016/j.adolescence.2016.12.002.
Velempini, Mthulisi and Phillip Nyoni. “Privacy and User Awareness on Facebook.” South African Journal of Science, vol. 114, no. 5-6, 2018, pp. 27–31, https://doi.org/10.17159/sajs.2018/20170103.
Zhang, Renwen. “The Stress-Buffering Effect of Self-Disclosure on Facebook: An Examination of Stressful Life Events, Social Support, and Mental Health Among College Students.” Computers in Human Behavior, vol. 75, 2017, pp. 527–537, doi.org/10.1016/j.chb.2017.05.043.
One of the most recently reported-on events are the confirmation hearings of Judge Ketanji Brown Jackson, as she becomes the first ever African American female nominee to the United States’s highest judicial court. Her hearings are currently being discussed everywhere from mainstream news shows to TikTok, highlighting the trend of increased public interest in the Supreme Court and increased personality politics that have breached the Court in recent years.
Unlike many similar institutions around the world, the Supreme Court of the United States is an inherently political one, where Justices are easily placed on the Liberal-Conservative scale. It is now seen as an accomplishment of the President to place someone on the bench– not because it is an opportunity for greater education and stronger debate, but because it increases the likelihood of the President’s policies passing easily through the judicial branch. Retirement of Justices is now strategically planned, with Justices of a certain political leaning delaying or expediting their retirement in order for it to occur under a President they support, so that their replacement would be of a similar ideology. When Justice Ruth Bader Ginsburg passed away, Republicans rushed to pass Justice Amy Coney Barrett’s appointment, as it was just a month before the 2020 election and former President Donald Trump risked losing the opportunity. This is an inherent risk with lifetime appointments, as electing Justices of roughly similar ages means that there are often multiple vacancies opening up all at once, and some Presidents are given the opportunity to appoint multiple Justices. In four years, Presidents Trump and Richard Nixon appointed three and four SCOTUS Justices, respectively, whereas both Presidents Barack Obama and George Bush Jr. each appointed just two in their eight years (and no vacancies opened up during President James Carter’s term). The opportunity to elect a Supreme Court Justice was a rare one, so Presidents needed to take the chance to appoint someone who will support as many of their policies as possible.
Never before has such scrutiny been placed on a Supreme Court nominee as that on Ketanji Brown Jackson. Her initial naming was controversial, as many took issue with President Joseph Biden’s campaign statement that he would appoint “the first Black woman ever nominated to the United States Supreme Court,” with some claiming that this undervalued the Court, arguing that “a nominee’s race or gender should not play a role in Biden’s selection process.” However, this argument is not unique in 2022, as in 1980, President Ronald Reagan made a promise to elect a female Justice, stating that he would appoint “the most qualified woman [he] can possibly find.” Whilst he failed to do so, with the first female Justice coming 13 years later with President William Clinton’s appointment of Justice Ruth Bader Ginsburg, Reagan’s campaign promise was not dissimilar to Biden’s, as it suggests nomination based on an underrepresented demographic (in this case gender). It is also important to remember that Reagan’s statement crosses party lines, and whilst not all of the outrage against Biden’s statement came from Republicans’, they were certainly the leading voice. Parties have become so polarised that they are now disagreeing with issues that their own party championed just 40 years ago, and this has concerning implications for the future of bipartisanship.
However, the arguments over Biden’s decision limits Judge Brown Jackson’s candidacy to a discussion just about race. Senator Ted Cruz questioned her on children’s books such as “Antiracist Baby” by Dr. Ibram X. Kendi, asking questions such as her opinion on critical race theory and if she “thought babies were racist.” Whilst critical race theory is a widely debated issue across the country right now, it is important to note that neither Justices Brett Kavanaugh nor Amy Coney Barrett were questioned on this topic, and certainly neither of their confirmation hearings involved scrutiny of children’s books. Senate Minority Leader Mitch McConnell said he would vote against Brown Jackson’s appointment, as she has refused to comment on the issue of adding seats to the Supreme Court, in agreement with Justice Coney Barrett, as she too had refused to comment on the issue. However, when speaking of Amy Coney Barrett, Mitch McConnell stated that she was an “incredibly impressive jurist and highly qualified nominee.” Whilst it is far from surprising that a Republican leader would denounce a Democratic pick for the Supreme Court, it is vital that the arguments made against her are scrutinised and understood, just as those made against Republican picks must be as well. In a similar vein, there has been little discussion within mainstream news of how she is the most qualified lawyer of all those sitting on the Court. The following graphic has gone somewhat viral on social media, which compares Judge Brown Jackson’s legal history with the 9 other Justices.
Whilst there is no expectation of having to agree with Judge Brown Jackson, and indeed it would be both problematic and damaging to democracy if the Court only contained members who represented one ideology, experience is something which cannot be misrepresented or denied. In the same debate speech in which he announced his intention to elect a Black woman, Biden stated that “if I were Black, my success would have been a lot harder to achieve. And I know a lot of black people that if they were White it would have been a lot easier for them.” Not only does Judge Brown Jackson’s race not undermine her experience, but it may actually show more experience; she has worked in so many areas of the legal system because she was unable to skip stages, due to barriers in place due to her race. It would be unjust to minimise her nomination to a mere diversity pick with little standing, as her experience outweighs any discussion of her race.
The Supreme Court as an institution works best when it is diverse and varied. At its very core, its function is to scrutinise the workings of the government, and this will never work when unbalanced and biased. Whilst legal systems in other countries work with the core foundation of neutrality, the entire government of the US was created with the idea of ambition challenging ambition. Every Justice, just like every President and every Congressman, has their own personal views, and the system operates best when each opinion is challenged and picked apart by an equally represented, but opposite opinion. The presence of Brown Jackson, as a left-leaning voice on the Court, would merely replace Justice Stephen Breyer, who is leaving the Court, and therefore the Court would still be politically unbalanced, with six of the nine Justices – Clarence Thomas, Samuel Alito, Neil Gorsuch, Amy Coney Barrett, Brett Kavanaugh, and John Roberts – representing Conservative ideals. Whilst it would be politically beneficial for Biden to appoint a liberal Justice as he has done, it will still have little effect on the Court’s overall ideology. What Judge Brown Jackson does provide, however, is a wealth of knowledge and experience, and this can only improve the Court, as the healthiest thing in a democracy is well-educated representatives. Whilst her race undoubtedly allows her to have an important voice for a consistently underrepresented group, it would be unjust and unrealistic to say that she represents the views of every Black woman, just as it would be incredulous to think that race places a role in every decision she would make on the Court, especially considering the wide range of issues they rule on each year.
The intention of this essay is not to suggest that Ketanji Brown Jackson is a perfect candidate, or even that scrutiny of her should be easy. Senate confirmation hearings are supposed to be of great substance and hard questioning, as this is the only way to achieve the most accomplished Court possible. However, the questioning placed upon one Judge should be equal to that of another, and this is not being done. President Biden’s criticism that race should not be important when choosing nominees can only remain valid when it coexists with fair treatment under questioning, and therefore Judge Brown Jackson’s questioning should not be entirely centred around her race. By asking questions about antiracist babies and asking her to rate her religion on a scale of 1-10, we dismiss the real debate that should be occurring in regards to the Supreme Court– by having a highly politicised Court in which Presidents can only effect change in the instance of retirement or death, are we rendering the judicial branch of government inoperable and imbalanced, and how can we protect the Court from this? Will set term limits allow for a more structured and less random appointment process, so that Presidents use their appointing powers in equal measures, or will this defeat the Founders’ intentions when creating an effective Court?
Bibliography
Barabak, Mark Z. “Column: The architect of Reagan’s pledge to put a woman on the Supreme Court says it was all political.” Los Angeles Times, Feb 2022
Burtt, Kristyn. “Ketanji Brown Jackson Faced Some Astonishingly Stupid Questions About Racism From Ted Cruz.” SheKnows, March 2022
CBS News. “Full Transcript of the South Carolina Debate.” CBS, Feb 2020
Kaslovsky, Jaclyn and Andrew Stone. “Biden vowed to nominate a Black woman to the Supreme Court. It might be good politics.” The Washington Post, Feb 2022
McMillion, Barry J. “Supreme Court Nominations 1789 to 2020.” Congressional Research Service, March 2022
Mitch McConnell Senate Website. “McConnell Praises Judge Barrett and Denounces Attacks on Judicial Independence.” The Newsroom Remarks, Sept 2020
Quinn, Melissa. “Mitch McConnell says he opposes Ketanji Brown Jackson’s Supreme Court nomination.” CBS News, March 2022
Schwarz, Frederick A. “Saving the Supreme Court.” Brennan Center For Justice, Sept 2019
The incidence and mortality rates of cancer remain at an unreasonably high rate despite the existence of cancer therapies. In 2018, nearly 10 million lives were lost as a consequence of some form of cancer (NIH, 2020). That same year, almost 20 million novel cases of the pernicious disease arose (NIH, 2020). While anticancer treatments, such as chemotherapy and radiation therapy, are credited with increasing survival rates of cancer patients in the last 50 years, these anticancer therapeutics are coupled with unintended consequences. More often than not, survivors are free from malignant cells, but are left to manage chronic, adverse side effects. Maladies caused by the central treatment often require further medical care. Additional ailments arise because these anticancer agents are nonspecific in their targeting, leading to an inability to distinguish between healthy cells and their rapidly dividing, malignant counterparts. This has led to the development and engineering of drugs with the ability to identify healthy tissues while destroying the cancer, furthermore diminishing side effects.
Over the past decades, nanotherapy has emerged at the forefront of cancer treatment by offering the means to target tumors in a safer and more effective manner through its accuracy and selective delivery. This report will argue for the utilization and prioritization of nanotherapy by explaining how it works, how it has displayed significant benefits in early trials, and why it has the potential to be the superior option for cancer treatment.
The prefix “nano” describes one-billionth of a unit. Nanotechnology is the science that deals with a range of a few nanometers (nm) to several hundred nm, depending on its intended use. A “nanoparticle” is a suitable name as its sheer size can fit one-thousand particles end-to-end within the diameter of a single human hair. Other molecules quantified as nanoparticles include viruses and DNA. Nanoparticles fall under the umbrella of nanotechnology, expressed on an atomic, molecular, and supramolecular scale. Nanoparticles are applied as a cancer treatment, with precise, minimal side effects made possible by nanotechnology. When used to treat ill humans and animals, the nanomedical term for this manipulation of matter on a near-atomic scale becomes known as nanotherapy.
Three categories of nanoparticles exist: metal, non-metal, and composite. The ideal nanoparticle is based on conditions such as size and shape of the cancerous cells. Once the precise nanoparticle is determined, it is prepared using two delivery methods. Yu et. al state:
All the preparation methods of nanoparticles can be classified into two methods: bottom-up approaches and top-down approaches. The bottom-up approach is essentially through basic units (atoms, molecules and even smaller particles can be used as the basis for assembling the required nanostructures) stacked on each other to form nanoparticles, while the top-down approach is essentially where a whole solid material begins to decompose into nanoparticles (Yu et. al, 2021, 2).
Nanotherapy adopts a complex and unique ideology that begins with the loading of the nanoparticle to the patient. The different nanoparticle sizes and modes of delivery hit their greatest success rate once the patient’s needs are determined. The approach for nanoparticle synthesis calls for the optimum loading of either a drug, gene, or targeting ligand, which is “fired” at the cancer cell. The most common and aggressive nanomedicines include Abraxane (albumin nanospheres) and Doxil (PEGylated doxorubicin) which prevent cancer from dividing in the lungs, breasts, and ovaries. However, because each patient’s treatment is tailored to his or her diagnosis, nanomedicines and their dosage are unique to each patient. This is the essence of nanotechnology’s engineering: making anticancer agents that specialize in targeting the tumor while mitigating harmful side effects.
Nanotherapy has opened the door for a new era of cancer treatment thanks to numerous studies that demonstrate its great potential for combating cancer. Magnetic nanoparticles to treat mice with brain tumors revealed remarkable and promising findings. First, researchers discovered that the cancerous brain cells were eliminated with a 100 percent success rate, a result current therapies have never achieved. Second and most astonishing, the nanotherapy did not cause any adverse side effects in any of the mice. This outcome was reached through proper antibody loading, correct particle usage, and appropriate preparation methods (Northwestern, 2016). Employing this method also allows the receptors to be recognized and destroyed, thus eliminating threats to healthy cells and reducing side effects. The researchers’ work was praised, namely by lead scientist Dr. Maciej Leśniak. Dr. Leśniak suggested that nanotherapy could possibly be a panacea for a range of cancers. Leśniak stated, “I think this has applications to many types of cancers, from brain tumors to breast cancer. As long as there’s a specific target, you can take advantage of the nanoparticle’s mechanical properties” (Northwestern, 2016). Regardless of the anatomical location, tumors possess unique receptors which can be destroyed with the correct treatment. The research proved that when nanoparticles are properly chosen, loaded, and prepared, the cancer cells are specifically targeted, and unwanted side effects are slim.
Nanotherapy has also been shown to prevent specific cancerous outcomes from occurring. Researchers created a table showcasing positive outcomes of nanotherapy in malignant tumor patients. In the study, by adhering to the proper nanoparticle guidelines, loading, and preparation, the researchers discovered that nanoparticles in the subject cancer patient were found to have high enhancements of drug accumulation in the tumor (Sutradhar & Amin, 2014). In another patient where the cancer had metastasized, the secondary tumor was successfully destroyed with effective nanotherapy. The research clearly demonstrates the great potential for nanotechnology to be used to defeat cancer varieties.
Nanotherapy is unlike chemotherapy in that side effects are rare, and when they do occur, they are usually not caused by the nanotechnology itself (Zhang, et. al, 2019). Nanotechnology reduces traditional therapies’ side effects since its tailored style of treatment attacks soley the afflicted cells. Although nanotherapy’s side effects are not as common as its chemotherapy counterpart, patients who have been treated with Abraxane and Doxil, the only approved nanomedicines, have reported post-nanotherapy side effects of weight loss, nausea, and diarrhea. While Abraxane has shown to be efficacious and generally safe, Doxil has had many reports of unwanted adverse effects (Wu, et. al, 2017). “Adverse reactions are common after doxorubicin administration, including fatigue, alopecia, nausea and vomiting, and oral sores…Doxorubicin is also associated with significant cardiac toxicity, which limits the long-term use of the drug” (Johnson-Arbor & Dubey, 2021). However, a valid suspicion is that these problems may be from the chemotherapy drugs they contain. One explanation for chemotherapeutic drugs producing side effects is that cancer cells do not differ greatly from healthy cells. Because of their similarity, chemotherapeutic drugs like Abraxane and Doxil that kill cancer cells may also attack normal cells despite the implementation of a different mode of delivery. Therefore, conventional chemotherapeutic drugs could be phased out by less harmful nanotherapeutic agents to eradicate the causation of such unwelcome side effects.
Many cancer patients are recipients of chemotherapy and the incidental effects caused by the chemotherapeutic agents. Unlike nanotherapy, chemotherapy has little ability to be tailored to the patient’s specifications as it has adopted the proverbial “one size fits all” treatment. Patients generally receive the same prescribed conventional chemotherapy with little to no variation. Chemotherapy is engineered to be arbitrarily fired into the body and kill rapidly dividing cells, which subsequently results in a high mortality of healthy cells. Chemotherapy is not a guaranteed cure and is often shown to be ineffective in combating certain types of tumors. This is due to chemotherapeutic agents being too weak to reach the core of solid tumors and failing to eliminate any of the cancerous cells. Numerous “cycles” of treatment are performed in an attempt to destroy the cancer cells. Chemotherapy drugs are highly toxic and with each “cycle,” greater doses of radioactive particles enter the patient’s bloodstream. This can reduce life expectancy as well as produce possible deleterious side effects.
While many praise and are grateful for the life saving results of chemotherapy, in the long run, the often undesirable side effects may do more harm than good. I personally have seen the effects of chemotherapy through the experiences of one of my closest childhood friends. Thankfully, chemotherapy cured Steve of aggressive leukemia. While we all celebrated, his parents were mindful of the potential side effects they were advised of prior to their son’s treatment. Shortly after his final chemotherapy treatment, Steve began attending routine appointments, tests, scans, and procedures, the effects of which would remain with him for the rest of his life. Now in his late teens, Steve routinely visits many specialists to ensure his cancer does not return or metastasize, as well as making sure that his chances of reproduction are not being affected. The chemotherapy that was a blessing over a dozen years ago has also caused Steve high levels of anxiety, irrational behavior, mood swings, body image disorder, learning issues, and clinical depression. One cannot help but wonder: had Steve had the benefit of nanotherapy, would he perhaps not be facing these issues today?
Although cancer is one of the most dreaded and lethal diseases, there is a lack of awareness of current treatments for the cancer patient (WHO, 2022). Nanotherapy has strong potential to eliminate the lethal disease and decrease side effects that are produced by conventional therapies. Supported by research, nanotherapy could lead the way to the widespread implementation of the less harmful remedy for cancer patients. As further research and clinical trials are conducted, I am confident that these small particles will develop into safer, more effective life saving solutions.
Sutradhar, K. B., & Amin, M. L. (2014, January 16). Nanotechnology in cancer drug delivery and selective targeting. International Scholarly Research Notices, 2014, https://doi.org/10.1155/2014/939378
Wu, D., Si, M., Xue, H. Y., & Wong, H. L. (2017, August 16). Nanomedicine applications in the treatment of breast cancer: Current state of the art. International Journal of Nanomedicine, 12, 5879–5892. https://doi.org/10.2147/IJN.S123437
Yu, Z., Gao, L., Chen, K., Zhang, W., Zhang, Q., Li, Q., & Hu, K. (2021, May 20). Nanoparticles: A new approach to upgrade cancer diagnosis and treatment. Nanoscale Research Letters, 16(1), 88. https://doi.org/10.1186/s11671-021-03489-z
Zhang, Y., Li, M., Gao, X., Chen, Y., & Liu, T. (2019, December 17). Nanotechnology in cancer diagnosis: Progress, challenges and opportunities. Journal of Hematology & Oncology, 12(1), 137. https://doi.org/10.1186/s13045-019-0833-3
This essay examines maternal healthcare practitioners’ perspectives about and experiences with incorporating sex- and gender-based medicine (SGBM) into healthcare training at Stony Brook University, a leading medical institute in the United States. SGBM refers to the style of clinical practice that accounts for the ways in which biological sex characteristics and social constructions of gender affect healthcare outcomes. This method is particularly critical for women’s and reproductive healthcare providers because they routinely treat patients that experience gender and its unique interactions with other sociocultural factors. Within the wide range of literature discussing the need to integrate an SGBM lens into medical education, only a handful of scholars have examined why it is so difficult to actually accomplish. Building on this emerging body of evaluation research, I conducted several oral interviews with faculty at the Stony Brook Schools of Medicine and Nursing, discussing how they have reacted to this relatively new but essential field of medicine from the early 1990’s to today. The university has recently claimed that its health institutions are progressive both politically and practically, but I argue that “progressive” is an exaggerated description. Based on the interviews, instructors continue to face institutional as well as logistical barriers to incorporating an intersectional gender lens into their didactic and practical curricula. Furthermore, this case study offers insight into how practitioners can improve the ways they currently teach gender in order to produce more equity-conscious and diversity-respecting maternal care providers.
Full Text
“Learning is not attained by chance, it must be sought for with ardor and diligence.”
– Abigail Adams (“Abigail Adams,” 2019).
Introduction
Medicine, particularly medical education, has historically ignored the humanities and social sciences, especially intersectional gender and sexuality studies. Maternal and reproductive health scholarship that actually includes women as its subjects and researchers did not emerge until the women’s health movement rooted itself in American academia just over two decades ago. However, the field’s first fifteen years or so focused on biology-based differences between men and women with minimal regard for any individuals identifying outside the cisgender, heterosexual norm. Gender and sexuality only entered the conversation in the last five years, and even now, intersectionality is barely acknowledged. Medicine continues to primarily use the additive model, which considers various forms of oppression (sexism, racism, ableism, etc.) separately rather than examining how they operate inseparably (Kang et al., 2017).
And yet, intersectionality is more important than ever before, especially in the United States. The number of Americans who identify as a person of color and/or LGBTQ* grows every day (Jones et al., 2021; Jones, 2021). Therefore, it is imperative that medical providers understand how to treat their patients with respect for diversity in all its forms. As with any sustainable change, the process of removing heteronormativity from medical practices must begin with medical training. In this essay, I aim to provide a snapshot of where American medical education stands on the inclusivity stage. I will accomplish this by examining maternal, reproductive, and family healthcare practitioners’ perspectives about and experiences with incorporating sex- and gender-based medicine (SGBM) into education at Stony Brook University, a leading medical institute in the United States. These perspectives reflect the larger institution’s state of inclusiveness and progressiveness.
For reference, SGBM refers to the style of clinical practice that accounts for the ways in which biological sex characteristics and social constructions of gender affect healthcare outcomes. This method is particularly critical for women’s and reproductive healthcare providers because they routinely treat patients that experience gender and its unique interactions with other sociocultural factors. Building on this emerging body of evaluation research, I conducted several oral interviews with faculty at the Stony Brook Schools of Medicine and Nursing, discussing how they have reacted to this relatively new but essential field of medicine from the early 1990’s to today.
Stony Brook University has recently emphasized its “progressive” approach to healthcare, especially regarding women’s and LGBTQ* populations. In response, I argue that while the Schools of Medicine and Nursing are certainly more aware of SGBM than they were two decades ago, the university still lacks clear intersectional gender- and sexuality-inclusive training and approaches the education they do have in a non-inclusive, binary way. In this essay, I will provide historical context for my analyses by briefly summarizing key events in the trajectories of feminism, the Women’s Health Movement, and sex- and gender-based medicine (SGBM) in the late twentieth century. I will then conduct an in-depth analysis of my case study research and its implications. Finally, I will conclude by proposing potential ways for practitioners to improve how they currently teach gender in order to produce more equity-conscious and diversity-respecting maternal care providers.
Background
How maternal and reproductive medicine evolved with American politics
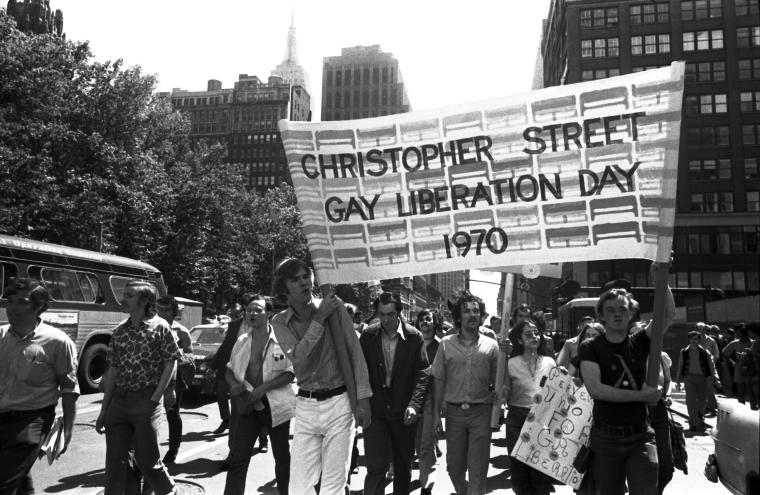
When Betty Friedan’s groundbreaking book The Feminine Mystique was published in 1963, America began to realize that many of its women were dissatisfied with simply being housewives (Churchill, 2020). After World War II, women were not especially keen on relinquishing the professional and financial freedoms they had found in the factories while the men were fighting overseas. Simultaneously, the Stonewall Riots in 1969 marked the birth of what is now commonly referred to as the modern LGBTQ* rights movement (Duberman, 1993). In the following decades, both of these marginalized groups would find themselves at the center of the global political and health stages.
Policy and health were particularly inseparable during this era. The 1990s saw what is now known as Third Wave Feminism, placing women’s experience at the center of American politics and “integrat[ing] an ideology of equality and female empowerment into the very fiber of [American] life” (Walker 400, 1992).Women delayed marriage into their mid-twenties, felt sexually liberated, and entered male-dominated careers (Yarrow, 2018).Yet, the fight for equality raged on in the political and medical arenas, clashing in landmark health-related historical events such as the Anita Hill sexual harassment hearings (Gross, 2021), Planned Parenthood’s fight against conservatives over abortion rights (Prescott, 2019), and the Violence Against Women Act of 1994 (“History of VAWA”).
In the same decade, the Women’s Health Movement was progressing with full-force activism: reproductive endocrinologist Florence Haseltine co-founded the Society for Advancement of Women’s Health Research in 1989, which helped to pass the Women’s Health Equity Act one year later and created the Office of Research on Women’s Health at the National Institutes of Health. In 1993, following the groundbreaking discovery that the HIV virus can pass from pregnant parent to fetus, Congress required the inclusion of women in NIH-sponsored clinical research trials (Liu and Mager, 2016). Prior to this mandate, women of childbearing age were considered too high-risk to participate in clinical research due to the possibility of pregnancy, severely inhibiting knowledge production about sex and gender in healthcare (Participant 3, 2021). It was these socio-political and medical paradigm shifts within women’s health research that gave rise to what is now referred to as sex- and gender-based medicine (SGBM). Within the wide range of literature discussing the need to integrate an SGBM lens into medical education, only a handful of scholars have examined why it is so difficult to actually accomplish.
How sex- and gender-based medicine was born
In the midst of this emerging field of women’s health intervention evaluation, Lorena Alcalde-Rubio et al. reviews 22 articles that evaluate clinical interventions aimed at “reduc[ing] variability in healthcare,” five of which focus on sexual and reproductive health (Alcalde-Rubio, 2020). The majority of the 22 evaluations supported standardizing protocols as a feasible method of systemic change, which is consistent with the faculty’s opinions during my interviews. However, Alcalde-Rubio’s review does not specify what types of protocols should be standardized and importantly notes that 15 out of the 22 evaluations did not utilize gender perspectives adequately. Further, the review significantly reflects a larger fault in medical academia: researchers often focus too much on the purely clinical aspect of change. When it comes to destabilizing social constructions that are ingrained in us and impact every aspect of human life both inside and outside of medicine, education plays a, if not the most, critical role in producing systemic change. In other words, we cannot fix the problem without addressing its roots. As such, I will primarily address the education aspect that Alcalde-Rubio et al. does not.
A 2005 Dutch study (Verdonk et al.) attempts to explore the potential for long-term change in medical education. Researchers concluded that a lack of guidelines, political ideology conflicts, and the educators’ own levels of dedication contribute to the gap between what should be taught and what was actually being taught. Further, certain factors must be present to successfully incorporate gender into medical training, including faculties’ personal experiences and motivations, practical support, and “executable” proposals for adjustment. This suggests that the Western medical educators were generally aware of the need for gender education in the 1990s, the decade during which many of my interviewees were medically trained here at Stony Brook. However, Verdonk, like many others in the field, conceptualizes gender as binary and essentialist.1 To make any meaningful progress, modern medical educators need to start deconstructing the gender binary and validating identities and sexualities beyond the cisgender, heteronormative ones.
Like Verdonk et al., Mary Rojek and Marjorie Jenkins (2016) examined medical schools, but this time in the United States. They surveyed faculty from medical schools that had already successfully integrated SGBM into their education. Their results suggested “it was important to involve all stakeholders… linking curricula to experiential learning and research. It was important to support faculty by providing them with educational resources” (Rojek and Jenkins, 2016). The majority of schools, though, are still behind in adding a sex- and gender-based lens to formal medical education. My research supports Rojek and Jenkins’ conclusions that formal institutional support is a crucial factor in determining integration success.
Also similar to Verdonk et al.’s case study, Hsing-Chen Yang examined the Eastern (Taiwanese) medical world’s perspectives about gender. Asian beliefs and social norms about gender are significantly different from Western ones, and even between individual Asian cultures themselves. Because Stony Brook’s Renaissance School of Medicine began accepting international applicants in 2014 (Medical School (MD) Applicant Profile, 2021), along with the majority of graduate students across the university identifying as people of color (Stony Brook University Fall Headcount, 2021), it is crucial to consider a diverse set of approaches to medical education. Because patient populations are now increasingly diverse—fueled by immigration and globalization—healthcare providers need to have a basic understanding of how gender functions in different cultures. Yang’s surveys found that healthcare professionals and teachers generally believe that sexism, gender awareness, gender equity, and patriarchy are among the most important to teach but this prioritization is not reflected in practice. However, the study omits two key factors: historical context and sociocultural context. Sexism, gender, and patriarchy have various meanings depending on the patient’s and the provider’s respective backgrounds. Therefore, Yang’s conclusions may be limited to predominantly Asian regions.
To see if Yang’s results holds true in Western medical culture, I came upon a 2010s-era study that revealed that American students also lack sex- and gender-based medical (SGBM) training, Majorie Jenkins et al. (2016) surveyed 1097 medical students across five major medical student organizations in order to examine institutional response to these findings. Jenkins’ survey suggests that while medical students are generally aware of SGBM’s existence, the majority do not receive adequate SGBM education at their respective medical schools. While it provides a solid look at what other American healthcare schools are doing about SGBM in relation to Stony Brook, Jenkins focuses solely on students’ perspectives rather than those of faculty, not accounting for logistical and institutional obstacles instructors face that students may not be aware of. I aim to fill this knowledge gap in this case study.
Methods
Stony Brook University
Stony Brook University (SBU) grew alongside the women’s movement. The university was founded in 1957 (“History and Mission”), and its Renaissance School of Medicine (RSOM) opened in 1971 (“History,” 2019). The RSOM currently houses 25 professional departments, including “Obstetrics and Gynecology,” which is an influential player in university progressive politics (“Departments,” 2019; Participant 5, 2021). One year after the RSOM admitted its first class, the SBU School of Nursing (SON) opened in 1972 (Strategic Plan 2016 to 2021, 2017). Graduate-level programs were gradually added in the following years, and the school’s first doctoral-level program, the Doctor of Nursing Practice (DNP) program, admitted its first cohort in 2007 (Participant 2, 2021). Now, Stony Brook’s Hospital is considered one of the best in the United States and boasts progressive and inclusive practices. This makes it an ideal institution to study the emerging field of sex- and gender-based medicine, especially considering its diverse student and faculty profile.
Sample
While gender undoubtedly affects all areas of health, obstetricians (OBs), gynecologists (GYNs), and nurses typically have the most direct patient contact with populations where gender is uniquely related to healthcare outcome (Participant 5, 2021). For example, maternal care and reproductive care specialists may see pregnant trans patients, same-sex couples with fertility concerns, and Black cisgender women, who have disproportionally higher rates of maternal mortality in the United States (“Working Together,” 2021). For this reason, I individually interviewed a total of six faculty at Stony Brook University, including three OB-GYNs from the Renaissance School of Medicine and three from the School of Nursing. Participants were recruited via email outreach based on whether they attended Stony Brook University for their undergraduate degree, graduate degree(s), residencies/fellowships, or any combination of those three. Each interview was approximately thirty minutes long and conducted over Zoom or phone call between the months of September 2021 and November 2021.
Table A. Participants’ Educational Backgrounds
Participant
Type of Clinician
Highest Degree Earned
Residency
1
Medical doctor
MD*
OB GYN*
2
Nurse practitioner and midwife
DNP*
N/A
3
Pediatric nurse practitioner
Ph.D.*
N/A
4
Family and acute care nurse practitioner
DNP*
N/A
5
Medical doctor
MD
OB GYN*
6
Medical doctor
MD*
OB GYN*
Key DNP – Doctor of Nursing Practice MD – Doctor of Medicine PhD – Doctor of Philosophy *Completed at Stony Brook University
Interview Questions
Educational Background
I asked the participants five main questions about various gender- and sexuality-related topics. The first question asked about the participants’ educational backgrounds, including where they earned their undergraduate degree(s), graduate degree(s), and where they completed their post-doctoral residency and fellowships if applicable.
Gender & sexuality education as a student
The second question asked about the participants’ experiences – or lack thereof – learning about gender as a student, including as a medical or nursing student and graduate-level nursing student or medical resident.
Current gender & sexuality education
The third question asked participants to compare their own student experiences to what current SBU students learn about gender. The fourth question asked about their experiences and opinions about teaching gender as a professor, including what challenges they may face and how they address them.
Institutional support
The fifth question asked participants if the university has offered and/or currently offers opportunities for faculty to further their own knowledge about gender and sexuality in healthcare, and if so, what types of opportunities and how helpful they were.
Results & Discussion
Participants’ own gender and sexuality training
None of the participants had any formal education about gender nor sexuality, with the exception of studying purely biological sex differences, when they were medical/nursing students. All participants received their first clinical degrees (BSN or MD) in the 1990s or early 2000s. At the time, SGBM was just beginning to grow as a legitimate field of medicine and was more commonly referred to as “gender-based biology” (Madsen et al., 2017).
For example, a few of the participants from both the RSOM and SON recalled learning about sex differences in symptom presentation and risk levels for certain conditions, such as the fact that men are more likely to have a heart attack while women typically show less obvious signs of a heart attack like pain similar to that of severe indigestion (Participant 3, 2021). Participant 2 recalled learning absolutely nothing about gender, especially its interactions with race and ethnicity. As a Black woman, she did not feel supported by the School of Nursing while earning her degree. Therefore, diversifying nursing education is particularly important to her, so a tremendous portion of the efforts to update the midwifery curriculum comes directly from her. This aligns with Verdonk’s 2005 findings, where a specific professor of Women’s, Gender and Sexuality Studies was an “important stimulus” and “trigger” person for SGBM integration. For Stony Brook’s midwifery program, Dr. Findeltar-Hines is the “trigger” person.
Another important consideration is that in the 1990’s, patients were often quite hesitant about revealing their gender identity and/or sexuality to practitioners (Participant 6, 2021). Furthermore, gender-affirming care standards, mostly relating to gender-affirming surgeries, did not exist until 1979 (Frey et al., 2017). The first major case study in hormonal puberty blockers, now a major treatment option for transgender, non-binary, and gender non-conforming pediatric patients, was not published until nearly twenty years later in 1998 (Cohen-Kettenis et al., 2011). Clinical progress took decades, and the curricula were trailing far behind as a result. This aligns with the Verdonk et al. case study of the Dutch medical center (2005), in which faculty’s personal experience and motivation was found to be a key factor in ensuring the success of gender education integration. Unlike the Dutch case study, though, Participant 2 acknowledges that gender exists on a spectrum and does not conceptualize it in mere binary terms, perhaps contributing to the Midwifery program’s progressive success in recent years. According to Participant 2, the program’s instructors have created a trans patient case study, use gender-neutral pronouns whenever possible, and are currently working on implementing gender/sexuality- and race-specific lectures.
This level of dedication to building gender-inclusive training is not consistent across the nursing and medical schools, however. While some participants recalled learning about “special populations” (Participant 4, 2021), which include trans and gay patients, it was from a very “cisgendered” perspective (Participant 1, 2021). This special population education was also added to the curriculum out of political pressure rather than student/faculty motivation. In the 1990s, HIV and AIDS awareness skyrocketed to the top of major health institutions’ priority list as the AIDS epidemic entered its “Middle Era” and gained international attention (Durvasula, 2018). This increased public health attention to women’s and reproductive health disparities, but commonly used terminology like the “4H Club [homosexuals, hemophilliacs, heroin users, and Haitians]” were homophobic and racist, essentially doing the opposite of increasing gender and sexuality awareness (Participant 3, 2021). In fact, prior to the AIDS epidemic, those who identified as female were prohibited from participating in medical research, so it’s not surprising that health practitioners and academics ignored gender education.
What current SBU students learn
Current SBU students learn more than participants’ did but the integration of gender and sexuality into the curriculum is slow. Challenges include time constraints (Participant 1, 2021), disparities in instructors’ own knowledge about the topics (Participant 1, 2021), and resistance from more traditional faculty (Participant 2, 2021). Ultimately, it is up to individual faculty to decide how much they want to adjust their curricula to include diversity education.
The Renaissance School of Medicine did not start internally pushing for inclusive education until two to three years ago (Participant 1, 2021; Participant 6, 2021), and since then, progress has been very slow. The majority of interviewees recognized the need for specialized gay and trans* education, but that was about the extent of their reported knowledge. Only one or two faculty mentioned non-binary and gender-nonconforming patients (Lian, 2021; Participant 3, 2021), and one mentioned the relationship between race, socioeconomic/citizenship status, and healthcare outcomes (Participant 6, 2021). None offered evidence of education that focuses on the vast variety of other gender and sexuality spectrums, including sexualities that are not strictly straight/gay/bisexual. Only one doctor mentioned how clinical placement affected patient populations. For example, attending physicians working at a Flushing, NY clinic might see more Asian patients while someone working in a “resident clinic” would typically see patients in less privileged socioeconomic groups. The resident clinics have more Hispanic and non-English speaking patients “by default” (Participant 6, 2021).
It is also worth noting that while a few participants mentioned race, gender, sexuality, socioeconomic status, and ability status separately, it was evident that all of them viewed gender and sexuality using an additive lens. The additive model considers systems of oppression to be individual entities rather than structures that cannot operate without one another. Intersectionality was undoubtedly an unfamiliar term, so interviewees were largely unable to answer questions about the intersections of identity factors like gender and sexuality. A potential cause of this issue is the lack of precise terminology in the broader field itself (Madsen, 2017).
The School of Nursing, however, began adding diversity and inclusion to its branding in 2017, which, coincidentally, is the same year the Midwifery Program appointed the first woman of color as its Director. In its academic success goals, the Strategic Plan 2016 to 2021 (2017) specifically lists “recruit diverse nursing faculty” and “expose [nursing students] to global health and healthcare disparities.” Since then, the midwifery program has been adapting lectures to use more inclusive terminology, such as saying “patient” instead of “woman” and “parent” instead of “mother.” Additionally, the program was the first in the SON to add a transgender-specific case study to the curriculum. As the program director noted in her interview, “Education is always evolving… We [educators] have to stay creative and innovative in order to get the basic education things that we want learned [by the students]” (Participant 2, 2021). This is both in agreement and in direct contrast with Yang’s Taiwanese survey of healthcare professionals and teachers regarding gender education expectations. Yang claimed that workplace sexism is a primary cause of the disparity between what instructors believe should be taught and what is actually taught about gender. She also argued that this same sexism prevents educators from viewing gender as a human issue rather than a “woman issue” (Yang, 2020). Participant 2 suggests that all educators must address gender education, including the traditionalists, and simultaneously expresses that workplace discrimination is not an excuse for lack of progress.
All faculty are required to retain clinical practice while teaching, and all participants hold additional leadership positions within their respective schools (Participant 4, 2021). Combined with minimal access to formal training, some traditionalists would say that faculty simply don’t have the time to educate themselves about gender so it is much harder for them to teach it (Participant 1, 2021). However, integration does not necessarily need to involve revamping the entire curriculum (Participant 3, 2021). Faculty could also incorporate gender diversity education into existing training, such as making a simulated patient a woman of color or a child with two mothers. Additionally, instructors could use case studies to emphasize a wide variety of lessons, such as Participant 2’s pediatric case study with a transgender (assigned female at birth) patient named “Timmy” (2021). This case study provides opportunities to practice using proper gender pronouns, learn about hormonal gender affirming treatments, and how to interact with parents of gender-diverse children. Across all interviews, participants said that they would like to improve the time dedicated to gender and sexuality education, so the motivation is there. These sentiments align with those of the students that Jenkins et al. surveyed in 2005, meaning formal course offerings have not improved much since then.
According to the participants, the students are the main driving force behind integrating gender and sexuality training into their healthcare studies. This result was also expected based on the Jenkins et al. survey (2005). On top of being very receptive and eager to learn about diversity, they even provide feedback asking to learn more (Participant 2, 2021; Participant 1, 2021; Participant 4, 2021). Depending on clinical placements, students also have the opportunity to interact with diverse patient populations (Participant 4, 2021), and at Stony Brook Hospital, residents consistently see high levels of diversity (Participant 5, 2021; Participant 1, 2021). While not all healthcare practitioners will work directly with gender-diverse patients, it is still extremely important for all medical providers to understand and be able to apply gender-inclusive theories. According to a recent 2021 Gallup poll, 5.6% of American adults, and one in six adults in Generation Z alone, identify as LGBT (Jones, 2021). Furthermore, the U.S. Census estimated that in 2019, over 36% of women were women of color, and this proportion is projected to grow to over 55% by 2060 (“Women of Color in the United States,” 2021). These statistics are particularly relevant to maternal and reproductive healthcare; therefore, it is critical that these healthcare providers are trained, at least on a basic level, in gender and sexuality studies (Participant 5, 2021).
Institutional support
Based on Verdonk’s 2005 study of a Dutch medical center, institutional support must be present in order to successfully incorporate sex- and gender-based education into healthcare curricula. This may be in the form of financial resources, guest lecture support, accessible educational resources, and visual/presentation support (Verdonk, 2005). With this in mind, I asked participants about how Stony Brook University supports its healthcare faculty in diversifying the curricula, if at all.
Using a binary gender lens
SBU as an institution provides some structured learning opportunities for faculty specifically about using an intersectional gender lens when practicing healthcare, but students and faculty want more. In terms of gender education, because the topic is so relevant to daily patient care for OB GYNs, a few formal lectures have been offered, and OB GYN residents discuss gender- and sexuality- related cases during grand rounds (Participant 5, 2021). For medical students, as of 2020, all SBU medical and dental students are required to take a “Transition to Medical and Dental School” course that talks about gender and diversity issues (Participant 1, 2021)
Using a heteronormativeLGBTQ* lens
In terms of LGBTQ* inclusivity, two of SBU’s major medical institutions, Stony Brook Medical Center and Stony Brook Southampton Hospital, scored a 100/100 on the Human Rights Campaign (HRC) Foundation’s 2020 Healthcare Equity Index [HEI] and were named LGBTQ Healthcare Equality Leaders (Healthcare Inequality Index 2020).2 According to Stony Brook, “[t]he HRC is the largest national lesbian, gay, bisexual, transgender and queer civil rights organization” (“Health Equality Leader,” 2021). However, the HRC has received a substantial amount of criticism for, despite its claims, failing to represent and advocate for LGBTQ* folks of color. Much of this controversy surrounded the Don’t Ask, Don’t Tell Repeal Act of 2010 (“H.R.2965,” 2010). In the months leading up to its official passing, the HRC used a disabled, gay veteran of color to promote fake inclusivity while it simultaneously “profited from the practice of diversity management” (Montegary, 2015). Further, the HRC has been called “cisgenderist” and white supremacist for several years (Johnson, 2011; Rosen, 2021). As such, their HEI rating may not have as much practical weight as Stony Brook claims.
Stony Brook University released an LGBTQ+ Health Needs survey in early summer 2021 and received over 1,218 responses from Long Island, NY residents as of September 30th, 2021. Its purpose is to “provide information critically needed by healthcare providers, social service providers, government officials and public health staff to expand service offerings and serve as effective advocates for LGBTQ+ people” (“LGBTQ+ Health Needs Survey”). Moreover, the survey was made available in both English and Spanish, increasing access to non-English speakers. Suffolk County alone is 20% Hispanic/Latinx, according to the U.S. Census Bureau estimates (“Quick Facts”).
Both the Stony Brook Medicine [SBM] and the School of Nursing [SON] have recently created committees to educate practitioners and spread awareness about gender-informed care. The SBM LGBTQ* advisor committee meets monthly and aims to establish a set of priorities for LGBTQ* patient care, as well as create a more welcoming environment for patients, practitioners, and staff (“Two Stony Brook Hospitals;” Participant 1, 2021). Additionally, the SON’s brand new IDEA committee [Inclusion, Diversity, Equity, and Access] aims to use student feedback to build a more inclusive learning environment (Participant 4, 2021; Participant 3, 2021). Faculty veterans accustomed to traditional academic politics may argue that committees are a poor use of resources, especially in higher education; however, as university administration researcher David Farris writes in “Not Another Committee” (2017), with regular communication, perceived equality among members, and actively focused leaders, committees can actually be quite effective. Nonetheless, it is still important to note that the learning opportunities produced by these committees, particularly at Stony Brook, are created for clinician audiences and are less advertised to didactic instructors (Participant 1, 2021).
Hiding behind generalized health inequity
Pre-COVID, nursing faculty went on a few retreats that focused on diversity inclusiveness, but it was addressed in a very general manner (Participant 4, 2021). Recently, Stony Brook Medicine ran a two-day conference entitled “The Long March to Equity,” which covered general healthcare disparities and their historical trajectories into modern day medicine (Participant 3, 2021). This was the only example mentioned by multiple participants, and I was unable to find any other examples.
One OB-GYN did mention Women’s Health Day, an annual conference at the Renaissance School of Medicine that focuses on various health issues (cardiovascular, eyesight, muscle, breast cancer, etc.) and is exclusively targeted at an all-female audience (Participant 6, 2021; “Women’s Health Day,” 2019). This participant noted that the OB-GYN department also hosts a women’s health clinic on the same day at which anyone can get a routine check-up for free. The department has also started a bi-weekly clinic that provides discounted services for uninsured patients (Participant 6, 2021). However, she also explained that basic needs such as transportation already inhibit many of their regular patients from accessing necessary healthcare appointments. While treating women for free or at lower rates is somewhat helpful, it does not address the issue of inequitable access in an intersectional way; essentially, these clinics are just a Band-Aid solution to a deeper, more complex problem.
Distinct differences between medical and nursing education
The next result I will discuss was unexpected but certainly worth noting. I found clear differences between the perspectives/openness of the medical doctors and nurses. While the medical and nursing models have been known to be incredibly separate for decades (Reed and Watson, 1994), I was surprised by how much the models impacted the providers’ perspectives on sex- and gender-based medicine. For reference, the medical model focuses on “diagnosis, treatment, and cure” and has been widely criticized for its “narrow and unsatisfactory view (Reed and Watson, 1994). On the other hand, the nursing model “offers a more humanistic approach to patient care” (Reed and Watson, 1994).
The Medical Model’s Shortcoming
During the interviews, OB-GYNs consistently steered their responses towards healthcare outcomes, while I found the important connection between education and patient experience to be missing. For example, medical doctor participants mentioned “sobering” maternal mortality statistics, grand rounds3 (Participant 5, 2021), and student feedback being important (Participant 1, 2021), but only one explicitly said they prioritized making patients “feel more comfortable… and heard” (Participant 5, 2021). Yet, is the entire reason for improving medical education to benefit the patients?
Additionally, all three of the OB-GYNs discussed referrals4 as a way to support gender- and sexuality-based diversity. While having and being knowledgeable about sufficient resources is absolutely necessary, it does not address the alarming fact that many maternal and reproductive care providers are entirely unfamiliar with the concepts of intersectionality and non-binary gender and sexuality spectrums. Patients should not need to see another doctor in order to be treated with bare-minimal respect and dignity.
The Nursing Model’s Humility
On the contrary, nursing faculty were much more open to discussing how their personal experiences and medical training affects the quality of care they deliver. For example, Participant 3 took a few gender studies courses during her undergraduate career at Stony Brook, which exposed her to “thinking about other cultures, other health belief systems that wasn’t just coming out of a textbook” (2021). This, she said, impacted both the way she teaches and the way she cares for her queer5 patients, particularly helping her grasp new concepts like non-binary genders and different cultural understandings of disability. Here, the connection between the importance of inclusive education and patient experience is clear. Further, Participant 4 explained how crucial it is for students to work with diverse patient populations during school so that when they enter the workforce as licensed providers, they will already have achieved at least a basic level of intercultural competence.
Faculty diversity
One final point I must discuss is that all six participants identified as women, and four identified as women of color (see Table A on page 9). This sample is not representative of the Renaissance School of Medicine’s and School of Nursing’s faculty at all. The School of Medicine’s Obstetrics and Gynecology department has 42 physician faculty, of which only 13 (about 30%) are women of color. Furthermore, not a single woman is a full professor (with tenure). The department Director and Chair, the two highest leadership positions in the department, are also both white men (“Our Providers,” 2021). Within the School of Nursing, there are 32 faculty, of which 27 (about 84%) are white women and 4 (12.5%) are women of color. There is only one woman of color who holds a director-level position (“Faculty & Staff Directory,” 2021). It seems, then, that the School of Nursing has not yet met its goal to “Recruit diverse nursing faculty” (Strategic Plan 2016 to 2021, 2017).
With these numbers in mind, it is not surprising that Stony Brook University is lagging behind when it comes to incorporating SGBM into healthcare training. The key “trigger person” suggested by Verdonk’s 2005 study is hardly present, which may be why the Midwifery Program is the most progressive program within the School of Nursing (Participant 2, 2021). Verdonk also notes that personal experiences are significant contributors to SGBM’s successful incorporation into medical education (2005). Therefore, because the School of Medicine’s OB-GYN department has two white men occupying its highest leadership positions, and because the School of Nursing only has one woman of color in a leadership position, gender-inclusive training may be extremely difficult to accomplish with the existing faculty structure.
Conclusion
In summary, when the participants, the majority of whom were initially medically trained in the late 1990s to early 2000s, were students, they did not receive any education about SGBM with the exception of purely medicalized topics. Today, Stony Brook medical and nursing students are taught more gender-inclusive curricula but not as much as faculty nor students would like. Participants expressed facing challenges such as finding time to create new content, lacking personal knowledge and familiarity with SGBM, and lack of institutional support in the form of formal, specific training opportunities. Overall, Stony Brook’s “progressive” practices and curricula continue to use a heteronormative lens and show no intentions of trying to dismantle it.
This case study provides a snapshot of the American medical system, which currently faces discrimination and disparities on both clinical and educational fronts. With more Americans openly identifying as LGBTQ* than ever (Jones, 2021), and with populations of color continuing to grow (Jones et al., 2021), addressing gender- and sexuality-based healthcare disparities is an essential piece to improving the health of the nation. If the COVID-19 pandemic has shown us anything, it’s that we are in a deep crisis, and we have been for decades, leaving marginalized groups with inexcusably inequitable care. One of the most effective ways to produce long-term, sustainable change is by educating future generations of providers. This is why it is so important to ensure our healthcare students are receiving, at bare minimum, adequate training on these topics.
Potential ways to improve SGBM education and ensure competency is 1) provide formal, structured training for educators; 2) incorporate SGBM into the didactic and clinical curricula using updated lectures, new case studies, more diverse patient populations, and inclusive simulations; 3) appoint more (qualified) individuals from marginalized groups to leadership positions; 4) allot more funding to gender- and sexuality-inclusive educational initiatives; and 5) continuously assess, collect feedback, and adjust accordingly.
To form a more robust understanding of the medical educators’ attitudes towards SGBM education, future research could involve more individual case studies of academic medical institutions and/or comparing multiple universities. Faculty and student demographics differ between schools and geographic regions, which may affect attitudes as well as financial and socio-political ability to incorporate SGBM into formal medical education.
Footnotes
1 Essentialists believe that certain groups (categorized by race and sex especially) have traits and behaviors that are determined by biological factors. Gender essentialism inherently supports gender inequality by viewing gender as a binary concept, i.e. man versus woman (Hepburn).
2 HEI LGBTQ scores were calculated based on four major criteria: 1) quality LGBTQ patient-centered care, 2) “Patient Services and Support,” 3) “Employee Benefits and Policies” including “transgender inclusive healthcare benefits,” and 4) Patient and Community Engagement” (Healthcare Inequality Index 2020 14).
3 “A grand round is a formal meeting at which physicians discuss the clinical case of one or more patients. Grand rounds originated as part of residency training wherein new information was taught and clinical reasoning skills were enhanced. Grand rounds today are an integral component of medical education” (Stöppler, 2021).
4 A referral is when a healthcare provider does not have sufficient expertise in a particular field and suggests that the patient see a more knowledgeable specialist in that field (“Referral,” 2021).
5 Here, I use the term “queer” to mean “not aligning with the norm” rather than the more conventional “non-heterosexual” meaning.
Acknowledgements & Disclosures
Thank you to Liz Montegary for providing guidance for my research process, and thank you to all faculty who interviewed with me. This research was not funded in any way by any institution and was a fully independent project.
“ACME Accredited Programs.” American College of Nurse-Midwives. portal.midwife.org/education/accredited-programs?reload=timezone. Accessed 14 Oct. 2021.
Alcalde-Rubio, Lorena, et al. “Gender disparities in clinical practice: are there any solutions? Scoping review of interventions to overcome or reduce gender bias in clinical practice.” International Journal for Equity in Health, vol. 19, 2020. doi.org/10.1186/s12939-020-01283-4.
Basmah, Safdar, et al. “Integrating Sex and Gender into an Interprofessional Curriculum: Workshop Proceedings from the 2018 Sex and Gender Health Education Summit.” Journal of Women’s Health, vol. 28, no. 12, 2019, pp. 1737–1742. doi:10.1089%2Fjwh.2018.7339.
Cohen-Ketenis, Peggy, et al. “Puberty Suppression in a Gender-Dysphoric Adolescent: A 22-Year Follow-Up.” Archives of Sexual Behavior, vol. 40, no. 4, 2011, pp. 843–847. doi:10.1007/s10508-011-9758-9.
“Departments.” Renaissance School of Medicine, 2019, renaissance.stonybrookmedicine.edu/about/departments.
Healthcare Equality Index 2020. Human Rights Campaign Foundation, 2020, hrc-prod-requests.s3-us-west-2.amazonaws.com/resources/HEI-2020-FinalReport.pdf?mtime=20200830220807&focal=none.
Jenkins, Marjorie, et al. “Sex and Gender in Medical Education: A National Student Survey.” Biology of Sex Differences, vol. 7, no. 1, 2016. doi:10.1186/s13293-016-0094-6.
Johnson, Karlee. “Equality for some: A critique of the Human Rights Campaign.” Daily Sundial, 9 Oct. 2011, sundial.csun.edu/45167/opinions/equality-for-some-a-critique-of-the-human-rights-campaign/.
Jones, Jeffrey. “LGBT Identification Rises to 5.6% in Latest U.S. Estimate.” Gallup News, 24 Feb. 2021, news.gallup.com/poll/329708/lgbt-identification-rises-latest-estimate.aspx.
Liu, Katherine, and Natalie Dipietro Mager. “Women’s involvement in clinical trials: historical perspective and future implications.” Pharmacy Practice (Granada), vol. 14, no. 1, 2016. doi:10.18549/PharmPract.2016.01.708.
Madsen, Tracy, et al. “Sex- and Gender-Based Medicine: The Need for Precise Terminology.” Gender and the Genome, vol. 1, no. 3, 2017, pp. 122–128. doi.org/10.1089/gg.2017.0005.
Montegary, Liz. “Militarizing US Homonormativities: The Making of “Ready, Willing, and Able” Gay Citizens.” Signs: Journal of Women in Culture and Society, vol. 40, no. 4, 2015, pp. 891–915. doi:10.1086/680333.
Prescott, Heather. “We Must Not Allow a Contraception Gap: Planned Parenthood’s Campaign for New Birth Control and Feminist Health Activism in the 1990s.” Technology and Culture, vol. 60, no. 3, 2019, pp. 816–832. doi:10.1353/tech.2019.0074.
Reed, Janice, and Don Watson. “The Impact of the Medical Model on Nursing Practice and Assessment.” International Journal of Nursing Studies, vol. 31, no. 1, 1994, pp. 57–66. doi:10.1016/0020-7489(94)90007-8
Rojek, Mary, and Marjorie Jenkins. “Improving Medical Education Using a Sex- and Gender-Based Medicine Lens.” Journal of Women’s Health, vol. 25, no. 10, 2016, pp. 985–989. doi:10.1089/jwh.2016.5948.
Verdonk, Petra, et al. “Integrating Gender into a Basic Medical Curriculum.” Medical Education, vol. 39, no. 11, 2005, pp. 1118–1125. doi:10.1111/j.1365-2929.2005.02318.x.
Walker, Rebecca. “Becoming the Third Wave.” 1992. The Essential Feminist Reader, edited by Estelle Freedman, New York : Modern Library, 2007, pp. 397–401.
Yang, Hsing-Chen. “What Should Be Taught and What Is Taught: Integrating Gender into Medical and Health Professions Education for Medical and Nursing Students.” International Journal Environmental Research and Public Health, vol. 17, no. 18, 2020. doi:10.3390/ijerph17186555.
Yarrow, Allison. “How the ‘90s Tricked Women Into thinking They’d Gained Gender Equality.” TIME, 13 June 2018, time.com/5310256/90s-gender-equality-progress/.
The following is a paper written for Stony Brook University’s Research and Writing in Psychology course (PSY 310) in which students were required to design an experiment and write a research paper based on it. It should be noted that all results and accompanying graphs, tables, and discussions, are imaginative and not based on conducted experimentation.
Abstract
The current study aimed to examine the effects of the congruence of parenting and teaching styles on adolescent students’ academic achievement. Teaching styles mirrored the parenting styles of authoritarian, authoritative and permissive. Sixty eighth grade students were randomly sorted into three different classes, each of which utilized a different style of teaching. It was hypothesized that students who experienced the same teaching style in the classroom as parenting style at home would achieve higher levels of academic success than those students who experienced different parenting and teaching styles. Academic achievement was measured by proctoring identical final exams to all students and analyzing the exam scores. Results showed that students who experienced the same parenting style and teaching style achieved higher final exam scores than students who experienced different parenting and teaching styles. These results support that students’ academic achievement in schools are affected by the similarity and differences that exist between their home and school environments.
Introduction
The many adults present in a child’s environment heavily influence their development and growth. Studies have aimed to look at the ways in which the style of parenting that a child’s guardians choose to follow may impact the child’s mental, emotional, and social development. Such parenting styles were typically identified as either authoritarian, authoritative, or permissive, whereby authoritarian parents show high control and little warmth, authoritative parents show high control and high warmth, and permissive parents show low control and high warmth towards their children (Walker, 2009). Additionally, besides the daily interactions children may have with their parents, their perception of and relationship with teachers while they are students have been shown to play a large role in their academic success (Alvidrez & Weinstein, 1999). It is on this premise that researchers have explored the extent to which parenting styles utilized in children’s home environments have impacted teacher-student relationships (Paschall, 2015). One study explored the effect of parenting styles in home environments on attachment issues and negative versus positive relationships with teachers, especially at a young age (Paschall, 2015). Studies such as this one have suggested that there may be an interconnected effect of different adults’ supervision approaches on children.
Teaching styles that instructors adopt in the classroom have shown many similar characteristics to the three types of parenting styles (Bassett, 2013). The ability to use the definitions of parenting styles to evaluate teaching styles was shown in one study in which college students were asked to evaluate teachers using the 30-item Parental Authority Questionnaire, also known as PAQ, which was a survey used to assess parenting styles in home environments. A few changes were made to the original PAQ; although the PAQ was created with the intention of analyzing parenting styles, scores using this survey were extended to teachers (Bassett, 2013). In a similar study, university students from Lander University were asked to read vignettes and describe the teachers in them as authoritative, authoritarian, or permissive, and then describe whether or not they would hire them. The students were also asked to identify the parenting styles they experienced at home, and the results were then analyzed to examine whether students’ preference in hiring teachers with different styles were related to the parenting styles the students experienced in their home environments (Bassett & Snyder, 2013). This study takes a more subjective view by asking the students for their perspective on which teaching style is preferable based on the students’ background.
When describing parenting styles, an authoritative approach to parenting has often been seen as most effective in regards to yielding positive results such as higher levels of social and emotional maturity (Bassett, 2013). Similarly, an authoritative teaching style was observed to be the most effective at increasing academic success in students (Walker, 2009). A study conducted by Walker in 2009 using fifth grade students and teachers described higher levels of success and even preference for teachers using an “authoritative” style. An important aspect to note is that while authoritative teaching styles were generally seen as more effective, there is not much research that exists analyzing how this effectiveness is impacted by the students’ home environments. The current study aimed to explore the connection between students’ experiences with parenting styles and teaching styles to determine whether or not experiencing the same or different styles at home and at school is most beneficial to the student.
The purpose of the current study was to determine how the relationship between parenting and teaching styles can influence adolescent students’ academic achievement at the end of an academic year. The teaching styles, categorized as either authoritarian, authoritative, or permissive styles, were designated to each experiment group with guidelines on how to maintain these definitions. Such guidelines included varying levels of leniency in regards to deadlines, supportiveness or consolement during struggles, and acceptance levels of disruptions in the classroom. Student achievement was measured using the final exam score at the end of the academic year. It was hypothesized that students who are instructed by a teacher adopting the same teaching style as the parenting style that student experiences at home will have excellent or high achievement while students who experience different teaching and parenting styles will experience acceptable or low achievement. By examining how similarities and differences in the student’s home and school environment impact their academic achievement through an objective lens, school environments can adapt to be better suited to students’ preferences and can more uniquely and effectively nurture their success.
Methods
Participants
Sixty students, 30 males and 30 females, entering eighth grade in September 2021 were recruited on a volunteer basis for this study. All participants were in the age range of 12-14 years old and were selected from Nassau County, Long Island, New York. Each participant also came from a household that contains two parents (or similar parental figure or guardian). Three mathematics professors from Stony Brook University’s Mathematics department were recruited to teach the classes. Participants were sorted randomly into three groups consisting of ten males and ten females each. All three classes of students were taught mathematics in accordance with the New York State mathematics curriculum, and all participants had to be able to read, write, and communicate proficiently in English.. All classes were held year-round at Garden City High School located in Nassau County.
Measures
Parental Authority Questionnaire (PAQ). All students were provided with a modified version of John R Buri’s Parental Authority Questionnaire (PAQ) from 1991 in order to gauge students’ assessments of the parenting style they experienced at home (Buri, 1991). The 30-item questionnaire asked students to rank statements regarding their parents using a 5 point Likert scale (Buri, 1991). While Buri’s questionnaire aimed to provide results regarding the mother and father’s parenting styles individually, the current study grouped the parents as a single entity and asked all 30 questions as they pertained to both parents or parental figures. For example, “As I was growing up I knew what my mother expected of me in the family and she insisted that I conform to those expectations simply out of respect for her authority” was modified to read “As I was growing up I knew what my parents expected of me in the family and they insisted that I conform to those expectations simply out of respect for their authority” (Buri, 1991).
Procedure
Each of the three groups of students were assigned to one of three teaching styles: authoritarian, authoritative, and permissive. Each of these styles was used by a predetermined teacher who was provided with guidance on how to implement their assigned teaching style as it pertained to leniency, supportiveness, and tolerance. For example, the permissive teacher was instructed to employ high levels of leniency with assignment deadlines, high levels of supportiveness when students expressed having trouble in class, and high levels of tolerance when students created disruptions during class time. The authoritative teacher was instructed to demonstrate low levels of leniency, high levels of supportiveness, and low levels of tolerance. The authoritarian teacher was instructed to display low levels of leniency, low levels of supportiveness, and low tolerance for disruptive behavior. Besides these guidelines, all three teachers were given identical lesson plans and content to teach each class.
In September 2020, all students were asked to complete the Parental Authority Questionnaire. Results were compiled and each student was then categorized into one of two groups without their knowledge. Group A consisted of students who were about to experience a similar teaching style to the parenting style they experienced in their households, and Group B was composed of students who would be experiencing different teaching and parenting styles in the classroom and at home.
All three classes of students were taught mathematics using the same lesson plan, co-developed by each of the three teachers. Throughout the school year, monthly observations of the class were conducted, during which the observers would note details regarding leniency, comfort, and tolerance demonstrated by each teacher for a day.
On June 10, 2021, all sixty students were presented with an originally created, cumulative 50-question multiple choice final exam in mathematics with answer choices A-D. Every test was taken on a Scantron sheet for unbiased grading purposes. All students, regardless of class, were provided with the same exam and took the exam in identical testing conditions at the same time and location. Individual scores from the exam were blindly calculated and measured on a scale in which scores higher than 90% showed excellent achievement, between 75%-90% signified high achievement, between 65-75% indicated acceptable achievement, and below 65% represented low achievement. These results were then analyzed as they related to each student belonging to Group A or Group B.
Results
In assessing students’ academic success it was predicted that students who experienced the same teaching and parenting style would display higher achievement than students who experience different teaching and parenting styles. Students were randomly placed into one of three classes (authoritarian, authoritative, and permissive), and students who reported having a parenting style similar to their teacher’s style were categorized as Group A, and those with parenting styles different than their assigned teacher’s styles were categorized as Group B. Results were compiled in order to support whether or not students who experience the same type of teaching style in the classroom as parenting style at home perform higher academically as shown by final exam scores.
Figure 1 shows a comparison of Group A and Group B students’ final exam scores in each of the three classes. A two-way ANOVA was used to examine the effect of group assignment in the three differently taught classes on academic achievement in eighth grade mathematics. Results showed a significant main effect of group assignment. Students who experienced the same teaching style in the classroom and parenting styles at home — Group A — achieved significantly higher final exam scores (M = 90.23, SD = 5.55) than students who experienced different styles in the classroom and at home (M = 77.87, SD = 5.73) classified as Group B F (1, 59) = 5.32, p <.05. Furthermore, based on the predetermined scale, a mean of 90.23 showed excellent achievement for Group A (falling between the 90th and 100th percentile), while students in Group B obtained a lower average final exam score of 77.87, signifying high achievement (falling between the 75th and 90th percentile). Additionally, results were calculated to analyze final exam scores for each teaching style classroom. Students in the authoritarian class obtained an average final exam score of M = 79.75, SD = 4.03. Students in the authoritative class obtained an average final exam score of M = 83.95, SD = 2.43. Students in the permissive class obtained an average final exam score of M = 83.5, SD = 4.47. No main effect was found for the style of teaching on academic achievement F (1, 59) = 2.36, p <.05.
Figure 1.
Average Final Exam Scores Across Three Math Classes
Note. This bar graph displays the comparison of Group A and Group B students’ final exam scores in three differently taught math classes.
Discussion
The present study was conducted in order to examine the effects of similarity or difference of teaching style and parenting style on students’ academic performance. It was hypothesized that students who were placed in a classroom with a similar teaching style as the parenting style they experienced at home would result in higher academic achievement. It was predicted that students with similar teaching and parenting styles, or Group A students, would show excellent (90-100%) or high achievement (75-90%) on the final exam in mathematics, while students who experienced different teaching and parenting styles, Group B, would exhibit acceptable (65-75%) or low (below 65%) achievement. Results showed that students in Group A showed excellent achievement while students in Group B demonstrated high achievement. These findings supported the hypothesis by showing that the level of similarity between teaching styles in the classroom and parenting styles at home (same or different) influenced students’ academic performance.
The current study used a novel approach to understanding the effect of different adult figures in adolescent students’ lives and how they work together to impact students’ success in education. Previous research has examined the relationship between the two styles, often focusing on the influence of parenting styles on teacher-student relationships, or vice-versa, showing support for the idea that the two are inter-connected (Paschall, 2015). Studies have also highlighted the success of one type of style over the other, often concluding that an authoritative style is seen as being more effective for the classroom and at home (Walker, 2009). While previous research has used a more subjective approach to understanding teaching and parenting styles and how they influence students by asking students to provide insight on preference and evaluation of the different styles, the current study aimed to take a more objective approach (Bassett & Snyder, 2013). The current study showed that students who experienced similar teaching and parenting styles had higher average test scores than those students who experienced different styles at home and in the classroom, providing quantitative support for the idea that both parents and teachers’ methods of supervision can impact students’ achievement together. While less focus was given on highlighting one style as more effective than the others, the study instead examined the relationship between school and home environments.
One strength of the current study was that it analyzed comprehensive success levels of students by examining average scores of a cumulative final exam rather looking only at final averages or at individual test scores throughout the year, which could be impacted by other factors such as homework completion or class participation, which may not accurately reflect content understanding (as it could be reflective of time constraints or student personality, respectively). Final exams were identical for each student, as was the curriculum, in an aim to make the content of the three classes uniform. Another strength of the study was categorizing students into Group A or Group B — depicting that the students were either going to experience the same or different parenting and teaching styles, respectively — without informing the teachers or students of these placements. This allowed for minimal influence or bias on the teachers’ or students’ parts in regards to academic performance or teaching methods.
One limitation of the study was the decision to make mathematics the subject to be taught by the three classes. Varying degrees of skill may have been present in each of the three classes, and no additional support classes (extra help, tutoring) were provided, thereby causing there to be a discrepancy between students who were previously skilled at mathematics and students who previously struggled with mathematics. Additionally previous research has shown that authoritative teaching styles were most effective in the classroom (Walker, 2009). This could mean that both Group A and Group B students could have been provided with the most ideal situations in the authoritarian style classroom when compared to permissive and authoritarian classes, indicating that an interaction may exist between the congruence of parenting and teaching styles and the specific parenting or teaching style itself.
The current study brought to light the importance of examining the many environments children and adolescents find themselves in and how they are connected to each other in impactful ways. This study suggests that students may be more comfortable and successful when they are learning in a familiar environment, and that the continuity that exists between home and school can impact students’ academic performance. Further research is needed to analyze other factors that can impact the students’ success, such as physical setting or other members of the environment (i.e., siblings vs. peers). These further studies can also incorporate the significance and effectiveness of home-schooled students and how the education system can be molded to better suit each individual child’s unique needs.
References
Alvidrez, J & Weinstein, R.S. (1999). Early teacher perceptions and later student academic achievement. Journal of Educational Psychology, 91(4), 731–746. https://doi.org/10.1037/0022-0663.91.4.731
Paschall, W.P., Gonzalez, H. Mortensen, J.A., Barnett, M.A., & Mastergeorge, A.M. (2015). Children’s negative emotionality moderates influence of parenting styles on preschool classroom adjustment. Journal of Applied Developmental Psychology, 39, 1–13. https://doi.org/10.1016/j.appdev.2015.04.009
Walker, J. M. T. (2009). Authoritative classroom management: How control and nurturance work together. Theory Into Practice. 48, 122–129. https://doi.org/10.1080/00405840902776392
See Sophia’s poster for the URECA 2021 Symposium here.
Abstract
In adolescence, females are more likely than males to experience an episode of depression (Hyde et al., 2008). Having a strong social network has been shown to protect against the development of depression and anxiety symptoms (Santini et al., 2015). In the U.S., adolescent social circles were largely disrupted during the initial phases of the COVID-19 pandemic. Although it has been suggested that higher perceived social support protects against poorer mental health (Magson et al., 2021), few studies have examined the potential association between relationship quality and mental health during the COVID-19 pandemic. In a sample of 104 12 to 18 year-old girls, the present study examined peer relationship quality prior to the COVID-19 pandemic and changes in depression and anxiety symptoms during March to April 2020. Relationship quality was measured with the self-report Network of Relationships Inventory – Relationship Qualities Version (NRI-RQV). Depression was measured with the Child’s Depression Inventory (CDI), and anxiety was measured with the Screener for Child Anxiety Related Disorders (SCARED). Across the entire sample, there was an increase in both depression (t = -4.88, p < 0.001) and anxiety (t = -3.07, p = 0.003) symptoms during the COVID-19 pandemic. In addition, pre-COVID-19 perceived closeness of friendships predicted changes in depression and anxiety symptoms during the COVID-19 pandemic. Specifically, greater same-sex (r = -0.29, p = 0.003) and opposite-sex (r = -0.21, p = 0.04) friendship closeness were inversely correlated with generalized anxiety symptoms. Opposite-sex friendship closeness was inversely correlated with depression symptoms (r = -0.26, p = 0.008). Parent-child relationships were also examined but were not associated with changes in mental health. Findings suggest that healthier peer friendships may serve as protective factors against depression and anxiety in adolescents. As vaccine distribution increases and social distancing policies become more relaxed, adolescents may be able to strengthen relationships that were impacted by the COVID-19 pandemic, contributing to improved mental health.
Adolescence is a critical developmental period for the emergence of sex differences in depression. By ages 13 to 15 girls are approximately twice as likely as boys to experience an episode of depression (Hyde et al., 2008). Prior research has taken a particular interest in the psychological mechanisms responsible for this shift, focusing specifically on girls.
For both sexes, strong social support networks have been shown to protect against the development of depressive and anxiety symptoms (Santini et al., 2015). In early 2020, when the initial phases of the COVID-19 pandemic began, these social networks were largely disrupted, especially for children and teenagers. The daily routine of interacting with classmates and peers at school was abruptly interrupted due to the shift to remote learning. During this time, research suggests that females in particular experienced a notable increase in depressive and anxiety symptoms (Hawes et al., 2021).
While some studies suggest that higher perceived social support protects against poorer mental health (Magson et al., 2021), few studies have examined the potential association between relationship quality and mental health during COVID-19. The present study examined pre-pandemic peer relationship quality and its potential for predicting depressive and anxiety symptoms during the early COVID-19 pandemic.
Hypotheses
The present study tested two hypotheses: 1) Individuals would display an increase in depressive and anxiety symptoms during the initial stages of the COVID-19 pandemic as compared to pre-pandemic symptoms, and 2) Both parent and peer relationships would inversely correlate with depressive and anxiety symptoms during the COVID-19 pandemic. In other words, healthier and closer relationships would be associated with fewer depressive and anxiety symptoms during COVID-19.
Methods
Participants
The sample consisted of 104 girls from an ongoing longitudinal study at Stony Brook University, the Impact of Puberty on Affect and Neural Development across Adolescence (iPANDA) project. This project is currently investigating the relationship between neural reward sensitivity and the development of depression. Eligibility included being assigned female at birth, aged 8 to 14, being literate in English, having no known medical or developmental disabilities, and living within 30 miles of Stony Brook University in Long Island, NY. One of the child’s biological parents also had to be willing to participate. The baseline sample consisted of 317 girls along with one of their biological parents. Baseline data collection was followed by two additional waves, each spaced approximately two years apart. The third wave was still in progress when the COVID-19 pandemic began in late March 2020, therefore not all of the participants had completed the data collection.
Measures
The iPANDA participants (N = 104) were included in the present study if they completed the included measures within the appropriate timeframes. One measure was completed prior to the pandemic (before March 18, 2020), and two measures were completed before and during (March 18, 2020 and after) the pandemic. The average time between the pre-COVID and during-COVID assessments was 55 weeks.
Network of Relationships Inventory – Relationship Quality Version (NRI-RQV)
The NRI-RQV questionnaire is a self-report measure that assesses participants’ relationships with their 1) mother or mother figure, 2) father or father figure, 3) boyfriend or girlfriend, 4) sibling, 5) best same-sex friend, and 6) best opposite-sex friend. The questions had Likert-style responses (1 to 6: 1 = low occurrence, 5 = high occurrence, 6 = not applicable) and were presented in matrix format with each relationship type. Questions were classified into one of ten scales; the five positive scales measured companionship, intimate disclosure, emotional support, approval, and satisfaction, while the five negative scales measured conflict, criticism, pressure, dominance, and exclusion. Each scale contained three items and was scored by averaging the item responses (Furman & Buhrmester, 2010). The present study focused on the Closeness score, which is the mean of the five positive scale scores, for the mother, father, best same-sex friend, and best opposite-sex friend relationships. Participants completed the NRI-RQV assessment pre-COVID.
Children’s Depression Inventory (CDI)
The CDI questionnaire is a self-report measure that assesses participants’ depressive symptoms (Kovacs, 1992). Scores were calculated by summing the item responses, which were Likert style (not often/doesn’t apply to me, sometimes/somewhat applies to me, very often/strongly applies to me). Participants completed the CDI assessment pre-COVID and during COVID.
Screen for Child Related Anxiety Disorders (SCARED)
The SCARED questionnaire is a self-report measure that assesses participants’ anxiety symptoms. Each item had Likert-style responses (0 to 2: 0 = not true, 2 = very true) and was categorized into one of five subscales: panic disorder or significant somatic symptoms, generalized anxiety disorder (GAD), separation anxiety disorder, social anxiety disorder, and significant school avoidance. A total sum score of 25 or above (out of 82) indicated the possible presence of an anxiety disorder (Birmaher et al., 1997). The present study focused only on the GAD subscale, where a sum score over 9 indicated the possible presence of GAD. Participants completed the SCARED assessment pre-COVID and during COVID.
Data Analysis
Using IBM®️ SPSS®️ Statistics (v.27) software, we conducted two paired samples t-tests to examine whether depressive and anxiety symptoms increased during the pandemic as compared to pre-pandemic. Further, we conducted follow-up partial correlations (controlling for pre-pandemic symptoms) to investigate the relationship between relationship quality and depressive/anxiety symptoms during the pandemic.
Results & Discussion
Figure 1. Pre-COVID-19 vs. COVID-19 SCARED GAD Subscale t-test
t = -4.88, p < .001
Figure 2. Pre-COVID-19 vs. COVID-19 CDI Total t-test
t = -3.07, p < .01
Table 1. Correlations between SCARED GAD (COVID-19), CDI (COVID-19), and peer relationships
COVID-19 SCARED GAD Subscale
COVID-19 CDI Total
NRI-RQV Best Same-Sex Friend Closeness (pre-COVID)
-0.287**
-0.080
NRI-RQV Best Opposite-Sex Friend Closeness (pre-COVID)
-0.205*
-0.259**
Controls: pre-COVID SCARED or pre-COVID CDI p < .05* p < .01** p < .001***
Table 2. Friendship closeness vs. COVID-19 symptoms regressions
COVID-19 SCARED GAD Subscale (β)
COVID-19 CDI Total (β)
NRI-RQV Best Same-Sex Friend Closeness (pre-COVID)
-.168**
.074
NRI-RQV Best Opposite-Sex Friend Closeness (pre-COVID)
-.018
-.124****
Controls: pre-COVID-19 SCARED and CDI; COVID-19 SCARED or CDI p < .05* p < .01** p < .001*** trending****
Results indicated support for the first hypothesis. Across the sample, participants had greater depressive (t = -4.88, p <.001) and anxiety (t = -3.07, p < .01)symptoms during the COVID-19 pandemic, as compared to pre-pandemic. However, results indicated only partial support for the second hypothesis. Pre-pandemic friendship closeness was associated with changes in anxiety and depressive symptoms; specifically, stronger pre-COVID same-sex friendship closeness uniquely correlated with smaller increases in anxiety symptoms during COVID (r = -.29, p < .01), while stronger pre-COVID opposite-sex friendship closeness uniquely correlated with smaller increases in depressive symptoms during COVID (r = -.26, p < .01). When controlling for pre-pandemic symptoms, pre-COVID same-sex friendship closeness still predicted changes in COVID anxiety symptoms (r = -.17, p < .01). Mother and father relationships were not found to be significantly predictive of changes in mental health during COVID.
Conclusion
Interpretations
It is possible that participants were more comfortable expressing worry to same-sex friends (girls), buffering against increased anxiety symptoms. Perhaps they shared feelings about missing friends or romantic interests at school. Findings also suggest that opposite-sex friends (boys) may have helped improve participants’ moods, buffering against increased depressive symptoms. The girls may have had a crush or two and were happier interacting with them, even if only virtually, while following stay-at-home orders.
Limitations
The sample was predominantly Caucasian and middle class, and from the Long Island, New York area. As such, the sample is certainly not representative of the entire United States, as the U.S. is much more racially and socioeconomically diverse. It is unclear whether or not these results would be similar for individuals of different backgrounds, since a variety of factors, including race, ethnicity, sex, and economic class, impact the degree to which people have been affected, either positively or negatively, by the pandemic (Center for Disease Control and Prevention). For example, Black and Indigenous Americans had the highest COVID-related death rates, while Asians and Whites had much lower rates (APM Research Lab Staff). According to the Pew Research Center, lower-income individuals were also more likely to report lost income and jobs due to the pandemic (Parker et al., 2020). As such, the present study’s sample may not have been affected by COVID-19 as much as other groups.
Further, all measures were self-reported, so participants may have been reluctant to share the full extent of their relationships and COVID-19 experiences. Another important consideration is that there was over a year, on average, between the pre-COVID and during-COVID assessments, meaning we could not account for potential significant life changes, such the death of a parent, losing touch with a friend, moving to a new place, and changes in relationship nature itself. Therefore, the present study’s results regarding pre-pandemic relationship quality may not be fully applicable to pandemic-era relationship health.
Future Directions
Overall, the results were largely what we hypothesized. Increased anxiety and depressive symptoms during the COVID-19 pandemic were evident across the sample and peer relationships predicted changes in mental health. Future studies should investigate these findings further and consider potential gender, race, and socioeconomic class differences that were not found in the present sample. Social factors like gender norms, double sex standards, race/ethnicity, and wealth may further influence the nature of adolescents’ social support networks and how they experienced the COVID-19 pandemic.
Birmaher, B., Khetarpal, S., Brent, D., Cully, M., Balach, L., & Kaufman, J. (1997, April). The screen for child anxiety related emotional disorders (SCARED): Scale construction and psychometric characteristics. J Am Acad Child Adolesc Psychiatry 36: 545–553. https://doi.org/10.1097/00004583-199704000-00018
Furman, W., & Buhrmester, D. (2010). Network of relationships questionnaire manual. Unpublished manuscript, University of Denver, Denver, CO, and the University of Texas at Dallas.
Hawes, M.T., Szenczy, A.K., Klein, D.N., Hajcak, G., & Nelson, B.D. (2021, January 13). Increases in depression and anxiety symptoms in adolescents and young adults during the COVID-19 pandemic. Psychological Medicine, 1–9. https://doi.org/10.1017/s0033291720005358
Hyde, J.H., Mezuklis, A.H., & Abramson, L.Y. (2008). The ABCs of depression: Integrating affective, biological and cognitive models to explain the emergence of the gender difference in depression. Psychological Review, 115, 291-313. https://doi.org/10.1037/0033-295x.115.2.291
Magson, N.R., Freeman, J.Y., Rapee, R.M, Richardson, C.E., Oar, E.L., & Fardouly, J. (2021). Risk and protective factors for prospective changes in adolescent mental health during the COVID-19 pandemic. Journal of Youth and Adolescence, 50, 44-57. https://doi.org/10.1007/s10964-020-01332-9
Kovacs, M. (1992). Children’s depression inventory. Multi-Health Systems, Inc.
Santini, Z.I., Koyanagi, A., Tyrovolas, S., Mason, C., & Haro, J.M. (2015, April 1). The association between social relationships and depression: A systematic review. Journal of Affective Disorders, 175, 53–65. https://doi.org/10.1016/j.jad.2014.12.049
The emphasis on STEM-related majors at colleges and universities has been aggressively fueled by the growing influence of educational systems and political propaganda (Wright). Job seeking websites—including Monster.com—stated that when it came to the highest-paid industries, “…No surprise, STEM majors—science, technology, engineering, and math—came out on top” (Monster.com). Based on salary figures from 2020, STEM-related careers earned on average 26.45% more than humanities-related careers (Monster.com). It makes sense that young people would be persuaded towards pursuing STEM related careers. But are there external factors pressuring college students away from the humanities?
In June 2020, the Australian government announced an economic reform package that was directed to lower the course fees associated for “job-relevant” courses, while at the same time, doubling the cost of programs in the humanities (Duffy). This raise puts the cost of humanities programs at the same level as medical schools; med school programs saw a 46 percent decrease, while humanities programs saw a 113 percent increase (Duffy). The Australian government stated that this economic reform package is aimed at increasing the employment rate for graduates, with employment growth in STEM-related fields expected to be significantly higher post-pandemic (Sears and Clark).
Australia is not the only country influencing the career track of college students. George Washington University’s (GW) president, Dr. Thomas LeBlanc, announced in 2019 that he planned to increase enrollment in STEM-related majors from 19 to 30 percent (Rich and Schwartz). As the undergraduate population shifts to STEM related programs, the number of STEM programs and courses will also have to increase in order to accommodate the increasing number of students. Katrin Schultheiss, chair of GW’s history department, worries that “…the changes will necessitate reductions in funding for non-STEM departments and result in a ‘radical shifting of resources away from non-STEM fields’” (Rich and Schwartz).
This push for STEM programs and graduates comes from a fear of losing the race for high-tech supremacy to China (Herman). Where does this fear originate from? In his 2013 State of the Union address, President Barack Obama said, “…Think about the America within our reach: A country that leads the world in educating its people. An America that attracts a new generation of high-tech manufacturing and high-paying jobs” (Archives.com). We can theorize that this fear derives from the American perception of the “Chinese Threat,” a fear that China will conduct “…brazen cyber intrusions” (FBI.gov) or continue to saturate our economy with global exports (Mack). Fear of the “Chinese Threat” did result in a significant increase in the number of STEM degrees; however, according to a 2016 Census Report, only 74 percent of those college graduates pursued STEM-related careers following graduation (Mand Labs).
Now, elementary schools are introducing STEM curriculums, including hands-on learning to promote STEM skills, hiring and retaining well-trained experts as teachers for STEM curriculums, and working to eliminate the gender pay disparity (Mand Labs); hoping to further increase enrollment in higher education STEM degree programs to meet the growing demand of STEM related careers. Whether or not these new strategies will be effective remains to be seen. What does the continued push for STEM degree programs mean for the humanities, in a world where humanities are needed more than ever? Increasing costs of attending humanities programs, coupled with budget cuts following the 2008 financial crisis, “…have resulted in some schools eliminating courses and degrees in subjects, such as foreign languages, art, and history” (Mullin). Deborah Fitzgerald, a professor of the history of technology at the Massachusetts Institute of Technology, says state schools are the first to eliminate humanities curricula: “…Their boards just don’t think they are important anymore” (Mullin).
The following article is a revised version of the original piece and does not include all photos. The full original article with all accompanying photographs can be viewed by downloading the PDF below (recommended, but viewer discretion advised).
American photographer Robert Mapplethorpe shocked the international art community in 1988 with The Perfect Moment exhibition at the Contemporary Arts Center (CAC) in Cincinnati, Ohio. Against politicians’ desires, the CAC decided to display Mapplethorpe’s work even though the Corcoran Gallery of Art in Washington, D.C. cancelled the same exhibit only a few months earlier (Tannenbaum). The majority of Mapplethorpe’s photos were labeled obscene and pornographic, leading to criminal charges pressed against the CAC and its director at the time, Dennis Barrie. One of the most shocking was Rosie (1976), a photograph featuring a friend’s three year-old daughter sitting with her legs open, revealing her nude body beneath her dress. The trial took over a year, ending in acquittal and the public display of Mapplethorpe’s work at the CAC in 1990, just over one year after his death in 1989 (Mezibov).
Nude photography was one of Mapplethorpe’s specialties. Several of his portfolios featured the S&M and LGBTQ* communities in New York City, particularly in nude portraits (“Biography”). Many believe his intense focus on the nude body was an expression of his homosexuality. Rosie however, was one of only two photographs of nude children—the other, Jesse McBride (1976), featured a fully nude five year-old boy sitting on a chair. Both photos were taken with the children’s mothers’ permission but still received heavy backlash and criticism for being “pornographic” (Mezibov).
Ultimately, Mapplethorpe’s Rosie (1976) was not meant to be pedophilic, but rather a response to increasing radical American conservatism during the 1970s and 1980s. Its showcasing in The Perfect Moment exhibition (1988) challenged the limits of censorship and artistic freedom, reflecting the growing social phenomenon of hypersexualization that continues to define American media today.
Mapplethorpe lived in the heart of LGBTQ* activism in New New York in the 1970s. It was during this decade that the gay community began seeing representation in mainstream media, including movies that featured gay characters and the establishment of Gay Pride week. In 1973, the American Psychiatric Association stopped recognizing homosexuality as a mental illness, and the corporate world started prohibiting sexual orientation discrimination (Rosen). The LGBTQ* community saw tremendous strides in equality and justice advocacy.
It was during this time that Mapplethorpe became an icon for LGBTQ* folks. According to his friend and writer Ingrid Sischy, Mapplethorpe’s works purposefully focused on homosexuality in order to draw attention. His unapologetically direct photographs helped turn homosexuality from a shameful secret into a proud identity (Sischy).
However, the AIDS epidemic soon heightened homophobia in the 1980s. Mapplethorpe heavily focused on black male nudes, a clear expression of his homosexuality, making him a prime target for censorship. Republican Senator Jesse Helms was especially offended by Rosie and hyperfocused on Mapplethorpe’s homosexuality, AIDS-related death, and interracial photographic subjects (Adler, Meyer). In 1989, Helms convinced the deciding congressional committee to pass a bill prohibiting the National Endowment of the Arts (NEA) from funding the Institute of Contemporary Art (ICA), which organized the original Perfect Moment exhibit, for five years (Adler, Tannenbaum). He did so by lying about the photographs he saw firsthand at The Perfect Moment and distributing copies of four of them to the other committee members (Meyer).
At the time, Senator Helms’ arguments reflected those of a growing conservative movement. His outrage about Rosie was less about the photograph itself and more about the artist. Furthermore, his push for censorship was less about Rosie’s exposed body and more about silencing the LGBTQ* community, including proudly gay folks such as Mapplethorpe. In his attempts to “cordon off the visual and symbolic force of homosexuality, to keep it as far as possible from [himself] and the morally upstanding citizens he claim[ed] to represent,” Helms ironically brought even more attention to it (Meyer 134).
Some supported censoring Mapplethorpe’s work by claiming he was a pedophile and child abuser, but neither Jesse nor Rosie recall him as such. As adults, both reflected on their portraits proudly (Adler). As censorship lawyer Edward de Grazia wrote regarding the Mapplethorpe case, “art and child pornography are mutually exclusive… no challenged picture of children having artistic value can constitutionally be branded ‘child pornography’ or ‘obscene’” (de Grazia 50). Though it was ultimately deemed non-pornographic after the Mapplethorpe trial, Rosie was only the beginning of a political push to seize funding from the arts, particularly the radical works such as Mapplethorpe’s, following several rising liberal and conservative movements in the previous decades.
Historical Context: Radical Conservatism and the Sexual Revolution
During the 1970s, the LGBTQ* community became more vocal, allowing gay men such as Mapplethorpe to be more openly accepted in the art world. In response, movements such as the New Right and the Christian Right emerged, led largely by American evangelicals claiming that homosexuality was morally sinful (“The New Right”). Mapplethorpe’s very existence contradicted traditional conservative values, and he could never align with socially-accepted heteronormative culture.
In fact, the Rosie controversy emerged during a new wave of conservative outrage that began a few years earlier in 1987, when Andres Serrano’s Piss Christ was awarded $15,000 by the partially NEA-funded Southeastern Center for Contemporary Art (Meyer). Along with many other Republican Christians, Senator Helms was deeply offended and embraced the opportunity to denounce another artist who defied traditional conservative values when The Perfect Moment debuted in 1988. At that point, Helms’ focus shifted from Serrano’s critique of religion to Mapplethorpe’s expressions of homosexuality, repeatedly calling his photographs “sick” (Meyer 137). In doing so, Helms used the art as a larger metaphor for homosexuality and AIDS, which he believed were plaguing and contaminating Christian-American society.
Andres Serrano, Piss Christ, Cibachrome print, 1987.
As a gay man, Mapplethorpe was not sexually attracted to females at all, so it would have been much easier for Helms to use Jesse McBride rather than Rosie in his rhetoric. It was the ongoing sexual revolution, which also contributed to the rise of far-right conservatism, that put Rosie in the spotlight instead. Rosie, then, can be interpreted as Mapplethorpe’s way of challenging traditional ideologies and aligning with the sexual liberation movement. Where he saw an innocent child, many conservatives such as Senator Helms saw the bare sexuality of a young girl. Movements such as the New Right could not view her as anything other than sexual with her genitalia exposed. Therefore, it was not Mapplethorpe who sexualized the child but the audience who saw her, revealing a culture deeply rooted in traditional domestic roles and gender spheres.
The 1960s and 1970s saw a rapid increase in women’s and sexual liberation. Nonheterosexual sex was brought to national attention as well, especially after the Stonewall Riots in 1969 (Kohn). Much of Mapplethorpe’s work reflected this new spotlight. Rosie, though, was unlike his trademark photographs of an interracial S&M community, yet it still gained significantly more attention. Despite the portrait subject being a White child, Rosie was one of the four photographs that Senator Helms distributed to his fellow Congressmen and Senators. The others were Mark Stevens (Mr. 10½) (1976), Man in Polyester Suit (1980), and Jesse McBride (Meyer). There were several other photos of naked men in The Perfect Moment, many considered far more pornographic than Rosie and Jesse McBride could ever be, but Rosie was not chosen by mistake. She reflected a different, but not unrelated, threat to Christian-American tradition: women’s liberation.
After the birth control pill hit the market in 1960, sexuality and sexual expression were no longer taboo subjects. Rates of premarital sex increased significantly while books such as Alex Comfort’s The Joy of Sex normalized conversation about sex (Kohn). For many, Rosie represented a new generation of sexually-liberated women. For conservatives like Senator Helms, this was an intolerable break from traditional gender roles, where men and women had defined, separate roles in society. The New Right movement believed the sexual revolution was destroying the American family structure, leading little girls like Rosie from domesticity to radicalism (“The New Right”). Rosie, then, was the epitome of everything wrong with women’s liberation for Helms. In distributing her photograph, he attempted to defy the new wave of feminism.
However, despite its many controversies, the Mapplethorpe censorship case was most defiant of artistic freedom. Following the case, American art critic Robert Storr wrote that “there are no ‘laws of decency’; certainly none that have any juridical standing with respect to art” (Storr 13). He further argued that censorship itself is the manifestation of widespread mistrust of the public’s ability to draw their own conclusions. In a nation founded on freedom of speech and expression, art essayists like Hilton Kramer, who deeply criticized Mapplethorpe’s work, and politicians like Helms ironically believed that common people should not and could not discern what was acceptable, particularly regarding art (Storr). Helms and Kramer used censorship to impose their own beliefs onto the general public, serving as a microcosm of strong conservative attempts to minimize the voices of non-traditional values.
Robert Mapplethorpe exhibition, 2018, Gladstone Gallery, 515 West 424th Street, New York, NY 10011
When such defiances of conservatism emerged, they were immortalized in the form of art through Mapplethorpe and other “radical” artists like Serrano. In the heat of America’s changing society, Rosie became a monumental representation of true freedom: freedom of artistic expression, freedom of sexual expression, and the freedom of perspective. Politicians, however, disagreed over what freedoms should receive public funding. Helms and his fellow White Christian American conservatives believed that the NEA should not fund art that offended them based on “their assault on social constructions of sexuality, race, and spirituality” (Atkins 33). Once again, the majority group was attempting to impose their beliefs on the rest of society, a perfect example of censorship at its core.
Mapplethorpe’s case was significant but not the first. Works by LGBTQ* folks, people of color, and those with “dangerous” political views have been consistently marginalized. For example, Diego Rivera’s Portrait of America mural at Rockefeller Center was destroyed in 1933 because its center featured Vladimir “Lenin” Ulyanov, former leader of the communist Soviet Union (Atkins). In 1934, Paul Cadmus’ The Fleet’s In was removed from the Corcoran Gallery of Art—the same gallery that cancelled The Perfect Moment in 1988—because the Franklin D. Roosevelt administration requested it (Atkins). This was only a small part of FDR’s anti-gay legacy: during his time as Assistant Secretary of the Navy, FDR helped run a sting operation in Newport, Rhode Island in 1919, resulting in the arrest of over 20 Navy sailors for homosexual activity (Loughery). In 1981, after strong advocacy from Hilton Kramer and other conservative critics, the NEA stopped funding individual art critics because many of them were leftist (Atkins). Clearly, the Mapplethorpe case followed decades of conservative attacks on art.
Some believe the most pressing issues surrounding Rosie were Rosie’s age and exposed body. There were certainly multiple other artists photographing naked women at the time, like Don Herron and his Tub Shots series, who received little criticism for the nudity. In fact, nudity itself has never been an issue in art; some of the most famous and public classical works portray naked Romans, Greek gods, and biblical figures, like Michelangelo’s David and Sistine Chapel ceiling. In fact, nude boys were not an issue either, as seen in works like Thomas Eakins’s Boy nude at edge of river (c. 1882) and John Singer Sargent’s A Nude Boy on a Beach (1925).
The fact that Rosie was a girl was not the most significant factor either. During the 1970s, when the Rosie photograph was taken, the United States saw a rapid increase in explicit advertisements, particularly those with women only partially dressed or in full nude. One 1993 study revealed that the number of purely decorative female roles in ads increased from 54 percent to 73 percent from 1959 to 1989 (Busby and Leichty). A 1997 study found that over a 40-year period, 1.5 percent of popular magazine ads portrayed children in a sexual way, and of those ads, 85 percent depicted sexualized girls, with the number increasing over time (O’Donohue et. al). Even in the 1970s and 1980s, the sexualization of young girls was certainly nothing new. Advertising industries had been doing this for decades before the Rosie controversy started in 1988. In fact, they still do.
“Love’s Baby Soft. Because innocence is sexier than you think,” magazine advertisement, 1974–1975.
The hypersexualization of both women and children in the media is quite common now. As National Women’s Hall of Fame activist Dr. Jean Kilbourne reveals in So Sexy So Soon, corporations use sex and sexiness to advertise to children at increasingly younger ages—and they are alarmingly successful. Dangerously unhealthy standards of beauty define sexiness as the most important aspect of a woman’s identity and value. The sexual liberation movement of the 1960s and 1970s has turned into a hypersexualized culture, where children as young as Rosie are exposed to sex in songs, TV shows, advertisements, and social media (Kilbourne and Levin). Like the conservatives’ reaction to Rosie in 1988, young girls are now seen in a sexual way before they are seen as simply children.
Therefore, like the basis of Helms’ original arguments, the outrage and controversy surrounding Rosie was less about the photograph itself and more about the artist and what the artist represented. Mapplethorpe’s identity and lifestyle contradicted many traditional conservative values: he was homosexual, engaged in S&M, photographed interracial couples, and eventually died of AIDS. Rosie herself said she did not view her portrait as pornographic and could not understand why others thought it was. In fact, in a 1996 interview with The Independent, Rosie recalled her mother making her put on a dress just before the photo was taken, and immediately after, she took the dress off. Ironically, she noted that “if it had been a small [nude] boy, maybe this furore would be justified; Robert [Mapplethorpe] wasn’t interested in girls anyway” (Rickey). Jesse McBride, which is exactly that, received even less backlash than Rosie.
Helms, then, used Rosie against Mapplethorpe not because he thought it was pornographic, but because of all Mapplethorpe’s works, Rosie garnered the most conservative support for censorship. He could easily use the classic damsel in distress situation by painting Rosie as a helpless little White girl in need of protection from a dangerous gay man, with emphasis on Mapplethorpe’s homosexuality. It wasn’t Rosie’s age, nor her exposed body, that angered Helms: it was Mapplethorpe.
The Rosie controversy was just as relevant in 1988 as it is now. It continues to pose crucial questions, challenging the boundaries of art and the limits of censorship while highlighting the marginalization of LGBTQ* art, societal resistance to change, and hypersexualization of women and children. Ultimately, Rosie was not the creator of such outrage and conservative criticism, but the vessel exploited by powerful politicians to further their own agendas against Mapplethorpe and other LGBTQ* folks. The Mapplethorpe trial surrounding Rosie was the culmination of decades of liberal movements—including women’s liberation, the sexual revolution, and increasing attention to LGBTQ* voices—and the conservative responses to them. Despite the continuous controversy, critics consider Mapplethorpe, rightfully so, as one of the most influential American artists in the twentieth century. Rosie was last on public display in 2017 at the Guggenheim Museum in New York City.
Works Cited
Adler, Amy. “The Shifting Law of Sexual Speech: Rethinking Robert Mapplethorpe.” University of Chicago Legal Forum, vol. 2020, no. 1, 2020, chicagounbound.uchicago.edu/uclf/vol2020/iss1/2.
Atkins, Robert. “A Censorship Timeline.” Art Journal, vol. 50, no. 3, 1991, pp. 33–37. JSTOR, doi.org/10.2307/777212. Accessed 25 Jan. 2021.
de Grazia, Deward. “The Big Chill: Censorship and the Law.” Aperture, 5 May 1990, pp. 50–51. JSTOR, www.jstor.org/stable/24472936. Accessed 25 Jan. 2021.
Mapplethorpe, Robert. Ajitto. 1981. Solomon R. Guggenheim Museum, New York City. Guggenheim, www.guggenheim.org/artwork/2701. Accessed 28 Jan. 2021.
Mapplethorpe, Robert. Brian Ridley and Lyle Heeter. 1979. Los Angeles County Museum of Art, Los Angeles. LACMA Collections, collections.lacma.org/node/2155762. Accessed 28 Jan. 2021.
Mapplethorpe, Robert. Honey and Rosie. 1976. Los Angeles County Museum of Art, Los Angeles. LACMA Collections, collections.lacma.org/node/2233535. Accessed 28 Jan. 2021.
Mapplethorpe, Robert. Jesse McBride. 1976. Los Angeles County Museum of Art, Los Angeles. LACMA Collections, collections.lacma.org/node/2233522. Accessed 28 Jan. 2021.
Mapplethorpe, Robert. Ken Moody and Robert Sherman. 1984. J. Paul Getty Museum, Los Angeles. Getty, www.guggenheim.org/artwork/2740. Accessed 28 Jan. 2021.
Mapplethorpe, Robert. Rosie. 1976. Los Angeles County Museum of Art, Los Angeles. LACMA Collections, collections.lacma.org/node/2233440. Accessed 28 Jan. 2021.
O’Donohue, William, et al. “Children as Sexual Objects: Historial and Gender Trends in Magazines.” Sexual Abuse, vol. 9, no. 4, 1997, pp. 291–301. SAGE Journals, doi.org/10.1177%2F107906329700900403. Accessed 27 Jan. 2021.
Storr, Robert. “Art, Censorship, and the First Amendment: This Is Not a Test.” Art Journal, vol. 50, no. 3, 1991, pp. 12–28. JSTOR, doi.org/10.2307/777210. Accessed 25 Jan. 2021.
Tannenbaum, Judith. “Robert Mapplethorpe: The Philadelphia Story.” Art Journal, vol. 50, no. 4, 1991, pp. 71–76. JSTOR, doi:10.2307/777326. Accessed 26 Jan. 2021.
Brandon Chavez is a Class of 2024 undergraduate majoring in History. He enjoys learning about social and political issues in other countries & places around the world. He also enjoys learning about the challenges faced by indigenous populations.
***FALL 2020 CONTEST SUBMISSION***
”Suicide rates since 1960 in Micronesia (the U.S. Trust Territory of the Pacific Islands) have undergone an epidemic-like increase. This phenomenon is focussed narrowly within the 15-24-year male age-group”
(Rubinstein, 1983).
Family plays a quite significant role in Micronesian society. An individual’s self-esteem is very dependent on the acceptance and support of the family, more so than any other contributing factor. A firm place and role in the family is a source of self-esteem for an individual. The significance of familial relations and approvals are shown with one of Hezel’s statistics in his data: “Over 70 percent of all the suicides since 1960 were precipitated by conflicts within the consanguineal family” (Hezel, 55).
This phenomenon of high suicide rates among the male youth in Micronesia was first noticed by Reverend Francis Hezel, a Jesuit who was the director of Xavier High School in the Chuuk islands for nearly 18 years. Reverend Hezel wrote a magazine article about this phenomenon in 1977. Dr. Rubinstein, a researcher at Honolulu’s East-West Center, and Reverend Hazel later decided to research the issue further in the following years where they collected many facts about the situation but unfortunately did not come up with any solutions at the time. A later publication by Hezel in 1989 described the magnitude of the situation in Micronesia in comparison with the suicide rates of the United States: “The general suicide rate for Truk is 40 per 100,000. The rate for Trukese males between 15 and 25 is a startling 250 per 100,000. This is 20 times the youth rate in the United States” (Hezel, 1989).
Hezel observed that these suicides can be linked to small disputes between a young man and an older family member, like an older sibling or parent. Two examples were cited by Hezel to show his observation of the trend: one 13 year old boy hung himself after being scolded by his mother and a 16 year old boy also hung himself after his father refused to give him $1.
Another trend Hezel recognized was that the suicides would be clustered in groups; the death of one young man would often lead to suicides of others in the area.
When thinking about possible causes for these trends, Hezel initially thought that the process of modernization and its pressures clashing with traditional island societies was responsible for this phenomenon. Hezel and Rubinstein looked further into the issue and found that poor family relations were a common pattern with their research.
Hezel also described another insight into the issue that he gathered from his research:
“Rather than an impulsive act, we found the suicides were often the result of a longterm intolerable situation”
(Hezel, 1983).
Reverend Hezel’s insight reveals that these suicides in Micronesia are not impulsive, but that there is a cultural aspect to the situation, regarding a traditional island defense mechanism taken to an extreme. The word “amwunumwun” is used by the Chuukese to describe the behavior of young men using withdrawal to express shame or anger. Refusing to eat or being silent are examples of actions that these young men engage in when showing this behavior.
Reverend Hezel and Dr. Rubinstein believed that the strategy of amwunumwun became violent in the 1960s and 1970s where suicide might be considered the most extreme form of this behavior of bringing harm to oneself to save a relationship. A Chuukese suicide victim thought that being dead would repair more to a damaged relationship than if they were alive.In a later publication Reverend Hezel shed new insight on the suicide epidemic in the Chuuk islands (Hezel, 1989).
Figure 1
Note. Hezel found that anger was the leading cause of suicide in several islands in Micronesia (Chuuk, Pohnpei, Kosrae and Yap), the Marshall Islands and Palau (Hezel, 1989, p. 49).
Hezel also sought to find out the significance of the types of interpersonal and familial relationships that lead to suicide in Micronesia. Below is the table of his recorded data:
Figure 2
(Hezel, 1989, p. 51)
The table revealed that a relational disruption or conflict between a young man and his parents was often the most common cause of relational disruption that led to suicide. Hezel notes that in suicide cases that were led by disruptions in nonfamily relationships, the victim might break off familial ties because of the shame that might be bringing to their family and fear of what their family members’ reactions woud be. The victim was ashamed of actions that could offend their family and feared a consequential disruption in familial relations.
In 2007, Dr. Mao-Sheng Ran, a professor at the University of Hong Kong, reviewed pre-existing data on the characteristics of suicide in Micronesia.
Dr. Ran’s research found another phenomena that highlights the effect of mental health on suicide in Micronesia the effect of mental health on suicide in Micronesia compared with another country such as the United States.
Figure 3
(Ran, 2007, p. 83).
The bar graph above reveals an interesting and peculiar observation about the correlation between mental illness and suicide victims in Micronesia. Only 10% of suicide victims in Micronesia had psychiatric disorders, while 90% of suicide victims in the United States had mental illness. Dr. Ran states that: “Mental illness did not appear to be an important factor in Micronesian suicides. Most of the victims have had no serious delinquency problems, psychological abnormality, or psychosis” (Ran, 83).
Dr. Ran noted that intergenerational conflict was the most common cause that led to suicide and most suicides occured because of a conflict, misunderstanding or argument between a young victim and their parents or older relative.
The definition of anger in Hezel’s research is further explored in Dr. Ran’s review. Hezel’s publication in 1989 cited three distinct patterns of suicides which included anger suicides, shame suicides and psychotic suicides. It was previously mentioned in Hezel’s publication that anger suicides were the most prominent in Micronesian suicide cases, but this definition of anger adds a new understanding to the situation. Ran established that:”The definition of ‘anger’ was similar to the way Americans describe depression”(Ran, 2007, pg. 84). This definition of anger shows a cultural difference in how anger is defined in Micronesian society and American society.
The review also included several aspects and social changes that may be responsible for the high suicide rate in Micronesia. The first change is the expansion of a cash economy in Micronesia and the decreasing reliance on subsistence production. The production may be responsible for weakening the significance of clan and lineage activities. The decline in clan and lineage activities narrows social support for teenagers, increases reliance and dependence on parents, and increases parental-adolescent conflicts.The second change is the acceptance of suicide which can be attributed to this increase in suicide rates. As suicide becomes common among the youth, it became more acceptable and even expected.
According to Hezel, western solutions such as suicide prevention hotlines and counseling would not fully solve the suicide epidemic witnessed in Micronesia as the issue is not only psychological but also cultural. Dr. Ran offered several suggestions for future research to combat the issue. Ran suggests that there should be more surveillance on suicidal behavior in Micronesia, independent research on preventive and risk factors, and a longitudinal study on social and economic shifts affecting the male youth. Since there is not many mental health professionals available, Ran suggests that more individuals should be trained to counter the issue of suicide.
The Micronesian suicide epidemic is quite unique as the root of the issue is concerned more with the inter-generational conflict and socio-cultural elements found within Micronesian society rather than mental illness. Solutions to the issue and research on the topic cannot be treated in a western approach, as the act of suicide has shown to be woven into the youth culture of Micronesian society. Future studies, research, and clinical approaches must consider the socio-cultural elements of Micronesian society & family to make progress in combating the Micronesian suicide epidemic.
References
Hezel, F. (1989). Suicide and the Micronesian family. The Contemporary Pacific, 1(1/2), 43–74. Retrieved November 30, 2020, from http://www.jstor.org/stable/23701892